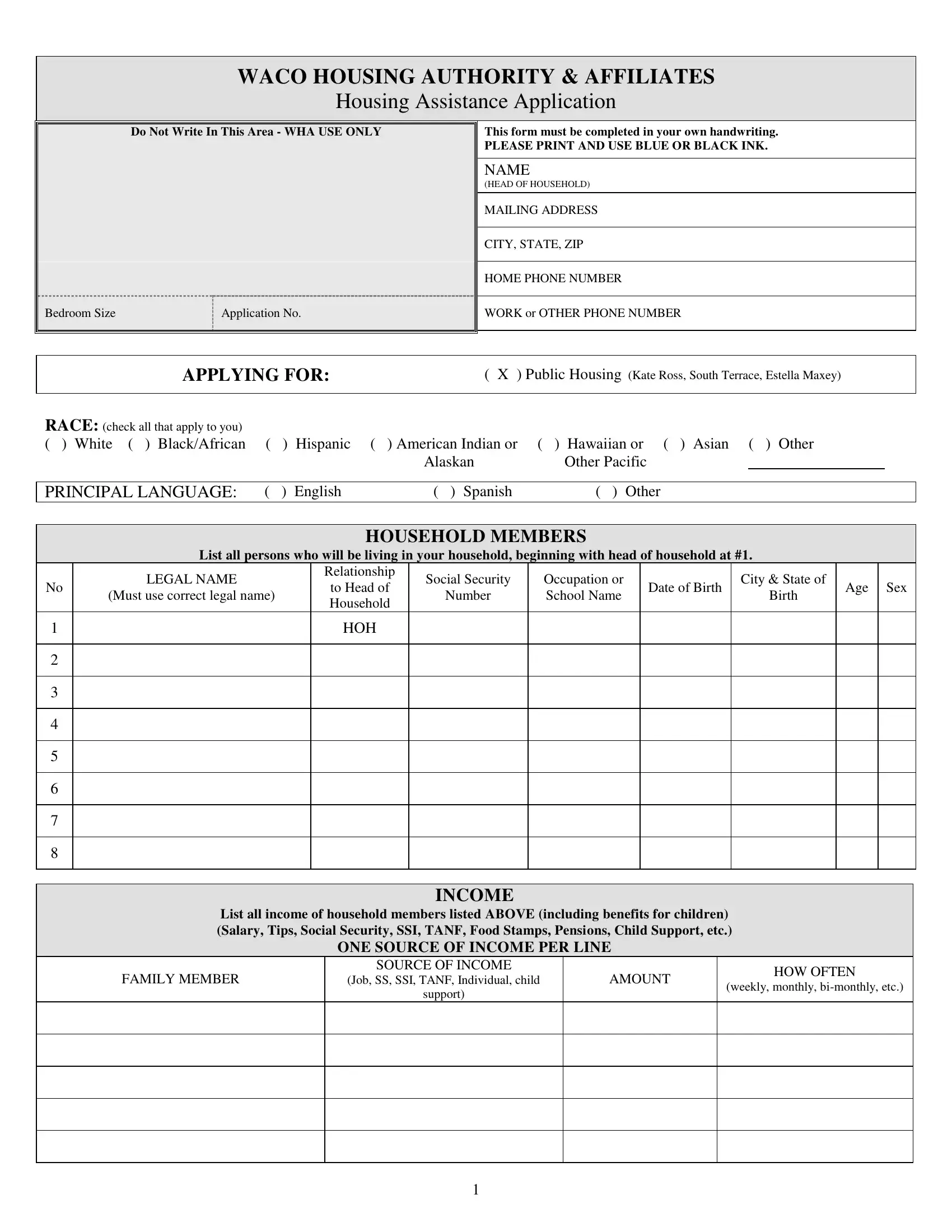
The Waco Housing Authority Application form stands as a detailed document designed for individuals and families seeking housing assistance in Waco, Texas. This comprehensive form requires applicants to manually fill in a multitude of sections with specific attention to clarity and accuracy, emphasizing the use of blue or black ink. From basic personal and contact information of the head of household to a detailed enumeration of other household members, the application delves into the specifics of each individual’s demographics, including race, principal language, and relationship to the head of household. Furthermore, it encompasses a broad spectrum of financial data, capturing varied sources of income, assets, and monthly expenses to accurately assess the applicants' financial status. Besides financial information, the document explores applicants' housing preferences, combining markers for public housing options with preferences that cater to veterans, the elderly, disabled individuals, victims of domestic violence, and those engaged in employment or training programs. The form meticulously gathers data on emergency contacts, personal references, residence history, and banking information, along with an in-depth inquiry into applicants' credit history and program integrity, probing into past housing experiences, criminal activities, and drug use. Through its rigorous and structured sections, the Waco Housing Authority Application encapsulates a thorough vetting process, tailored to prioritize and accommodate the diverse needs and qualifications of prospective housing assistance recipients.
| Question | Answer |
|---|---|
| Form Name | WACO Housing Authority Application Form |
| Form Length | 3 pages |
| Fillable? | Yes |
| Fillable fields | 108 |
| Avg. time to fill out | 22 min 25 sec |
| Other names | wacopha, housing authority waco texas, housing waco tx, waco housing |

WACO HOUSING AUTHORITY & AFFILIATES
Housing Assistance Application
Do Not Write In This Area - WHA USE ONLY
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Bedroom Size |
Application No. |
|
|
|
|
|
|
This form must be completed in your own handwriting.
PLEASE PRINT AND USE BLUE OR BLACK INK.
NAME
(HEAD OF HOUSEHOLD)
MAILING ADDRESS
CITY, STATE, ZIP
HOME PHONE NUMBER
WORK or OTHER PHONE NUMBER
APPLYING FOR:
( X ) Public Housing (Kate Ross, South Terrace, Estella Maxey)
RACE: (check all that apply to you) |
|
|
|
|
|
|
|
( ) White ( ) Black/African |
( |
) |
Hispanic |
( ) American Indian or |
( ) Hawaiian or ( ) Asian ( ) Other |
|
|
|
|
|
|
Alaskan |
Other Pacific |
|
|
|
|
|
|
|
|
|
|
PRINCIPAL LANGUAGE: |
( |
) |
English |
( ) Spanish |
( ) Other |
|
|
HOUSEHOLD MEMBERS
List all persons who will be living in your household, beginning with head of household at #1.
|
LEGAL NAME |
Relationship |
Social Security |
Occupation or |
|
City & State of |
|
|
|
|
No |
to Head of |
Date of Birth |
Age |
Sex |
||||||
(Must use correct legal name) |
Number |
School Name |
Birth |
|||||||
|
Household |
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
||
1 |
|
HOH |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
8 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
INCOME
List all income of household members listed ABOVE (including benefits for children) (Salary, Tips, Social Security, SSI, TANF, Food Stamps, Pensions, Child Support, etc.)
ONE SOURCE OF INCOME PER LINE
FAMILY MEMBER
SOURCE OF INCOME
(Job, SS, SSI, TANF, Individual, child
support)
AMOUNT
HOW OFTEN
(weekly, monthly,
1
INCOME INFORMATION
|
|
|
|
|
(These questions apply to all household members) |
YES |
NO |
|
Has anyone in your household applied for any benefits or money which is in the process of being approved? |
|
|
||||
|
|
|
|
||||
|
Does anyone outside of your household pay for any of your bills or expenses? |
|
|
||||
|
|
|
|
|
|
|
|
|
Are you entitled to |
( |
) Child Support |
( |
) Alimony ( ) Maintenance? |
|
|
|
|
|
|
|
|
|
|
|
Do you receive |
( |
) Child Support |
( |
) Alimony ( ) Maintenance? |
|
|
|
|
|
|
||||
|
Does anyone in your household receive an educational scholarship or grant? |
|
|
||||
|
|
|
|
|
|
|
|
MONTHLY EXPENSES
(From preceding month)
Rent |
|
Telephone |
|
Medical |
|
Credit Card |
|
|
|
|
|
|
|
|
|
Electric |
|
Auto Payment |
|
Cable |
|
Credit Card |
|
|
|
|
|
|
|
|
|
Gas |
|
Auto Insurance |
|
Insurance |
|
Loan |
|
|
|
|
|
|
|
|
|
Water |
|
Child Care |
|
Rentals |
|
Other |
|
|
|
|
|
|
|
|
|
CHILDCARE EXPENSES
|
Do you pay childcare expenses? |
( ) Yes |
( ) No |
|
||
|
|
|
|
|
|
|
|
If yes, list each child’s name below |
|
|
Amount |
Per (Month, Weekly, etc.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
HANDICAPPED ASSISTANCE EXPENSES
FAMILY MEMBER(S)
Amount
Per
(Month, Weekly, etc.)
Reason
MEDICAL AND UNUSUAL EXPENSES
ELDERLY FAMILIES ONLY
|
Amount |
Per (Month, Weekly, etc.) |
Medicare |
|
|
|
|
|
Other health insurance |
|
|
|
|
|
Regular payments on medical bills |
|
|
|
|
|
Regular payments for medicine |
|
|
|
|
|
Anticipated healthcare related expenses in the next 12 months |
|
|
|
|
|
Have you or anyone in your household ever owned a home or property?
( ) Yes
( ) No
ASSETS
List all assets of all “Household Members listed on page 1. (real estate, boats, mobile homes, etc.)
ASSETS |
CASH VALUE |
|
|
|
|
|
|
VEHICLES
How many vehicles does the family own?_________
Owner |
Make |
Model |
Year |
Color |
License # |
State |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2
HOUSING AUTHORITY OF THE CITY OF WACO, TEXAS
LOCAL PREFERENCE CLAIM FORM
For Public Housing and Section 8 Applicants
READ CAREFULLY AND CHECK ONLY THE PREFERENCES THAT APPLY TO YOU.
∙VETERAN’S PREFERENCE:
The head of household and/or spouse is currently a member of the Armed Forces, or the head of the household and/or spouse has an honorable discharge from the Armed Forces.
In the case of a divorce or legal separation, the head of the household or former spouse must provide the Waco Housing
Authority with documentation that the head or spouse has rights to benefits; there is no right to the veteran’s preference.
∙EMPLOYMENT PREFERENCE:
Families whose head of household or spouse is employed.
Families whose head of household or spouse has been given a bona fide offer of employment.
This preference does not require a minimum of income, but the family’s annual income cannot exceed current very low income guidelines by HUD. Must have a minimum of 20 working hours a week for Section 8 and 24 hours a week for Public Housing
No minimum length of time is required for the head or spouse to be employed. After
∙ELDERLY:
Head of Household or Spouse is 62 years of age or older.
∙DISABLED AND HANDICAPPED HEAD OF HOUSEHOLD:
This preference only applies to the Head of Household.
∙JOB TRAINING / SCHOOL PREFERENCE:
The head of household or spouse is currently enrolled and participating in a
Families where the head of household or spouse is a graduate of a
Head of Household is currently enrolled in educational programs working toward a degree. Must be a
∙DOMESTIC VIOLENCE PREFERENCE:
Household annual income cannot exceed current income guidelines by HUD
Must be certified by the Family Abuse Center that provides shelter or counseling to victims of domestic violence.
The Housing Authority shall determine that the domestic violence occurred recently (within 1 year) or is of a continuing nature.
The applicant shall certify that the person who engaged in such violence will not reside with the family unless Housing Authority has advance written approval.
The Housing Authority may deny or terminate assistance to the family for breach of certification.
FOR PUBLIC HOUSING RESIDENTS ONLY
TARGET UP AND OUT:
For families living in Public Housing who wish to move into the private sector and receive rental assistance through the
1.Families must have resided in public housing a minimum of one year, and participate in the Family
2.The family must participate in a job training program or attend an institution of higher learning or must maintain an earned income for a minimum of one year.
3.Families must be crime and drug free. This includes all persons on the lease.
4.Families must have a record of timely rent payments, for a twelve (12) month period. No balances left from month to month. Rent must be paid on or before the 5th of each month.
5.All
6.Families must have established a pattern of keeping their apartment and premises clean both inside and outside with no graffiti. This includes roof, yard, stairways and porches.
7.Must be in good standing with Public Housing at time of transfer.
8.Development managers must certify that the families have met the requirements.
I understand that my application is not a determination of eligibility for assisted housing / public housing. I will not immediately be offered housing, but will be placed on a Waiting List with other applicants, who may claim and/or are entitled to LOCAL PREFERENCE. The eventual extension of housing benefits will be based upon my place on the waiting list.
/ |
/ |
|
|
|
|
Social Security Number |
|
Applicant Signature |
|
Date |
|
3

EMERGENCY CONTACT
NAME
ADDRESS
PHONE NUMBER(S)
RELATIONSHIP
|
|
PERSONAL REFERENCES |
|
|
|
(relatives, close friends, employers, Pastor, neighbors, etc.) |
|
|
NAME |
|
PHONE NUMBER |
|
|
|
|
|
ADDRESS |
|
RELATIONSHIP |
|
|
|
|
|
|
|
|
|
NAME |
|
PHONE NUMBER |
|
|
|
|
|
ADDRESS |
|
RELATIONSHIP |
|
|
|
|
|
|
|
|
|
NAME |
|
PHONE NUMBER |
|
|
|
|
|
ADDRESS |
|
RELATIONSHIP |
|
|
|
|
RESIDENCE HISTORY
(List where you have lived for at least the last three years beginning with where you live now)
(If you live with someone else that pays the rent or owns the property, list that person as your landlord)
CURRENT STREET ADDRESS |
|
CURRENT RENT |
|
|
|
|
|
CURRENT LANDLORD NAME |
CURRENT LANDLORD’S PHONE NUMBER |
|
|
|
|
|
|
|
|
|
|
PREVIOUS ADDRESS |
RENT |
||
|
|
|
|
LANDLORD NAME |
LANDLORD’S PHONE |
NUMBER |
|
|
|
|
|
|
|
|
|
PREVIOUS ADDRESS |
RENT |
||
|
|
|
|
LANDLORD NAME |
LANDLORD’S PHONE |
NUMBER |
|
|
|
|
|
|
|
|
|
BANKING INFORMATION
List banking information for all “Household Members” listed on page 1. (checking, savings, credit union shares, annuities, stocks, bonds, CD’s, etc.)
Name of Financial Institution |
Type of Account |
Current Balance |
|
|
|
|
|
|
|
|
|
|
|
CREDIT HISTORY |
|||
|
|
|
|
|
|
|
CREDITOR |
|
PHONE NUMBER |
||
|
|
|
|
|
|
|
ADDRESS |
|
CREDIT TYPE (loan, credit card, car payment, etc.) |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
CREDITOR |
|
PHONE NUMBER |
||
|
|
|
|
|
|
|
ADDRESS |
|
CREDIT TYPE (loan, credit card, car payment, etc.) |
||
|
|
|
|
|
|
|
|
|
|
|
|
INPUT CLERK:
DATE:
4
PROGRAM INTEGRITY INFORMATION
(These questions apply to all household members) (All questions must be answered)
HAVE YOU, YOUR SPOUSE, OR ANY HOUSEHOLD MEMBER LISTED ON YOUR APPLICATION:
YES
NO
Been evicted or asked to move out of any rental property? |
|
|
|
|
If yes, Who? |
Where? |
When? |
|
|
|
|
|
|
|
Broken a rental agreement or lease contract? |
|
|
|
|
If yes, Who? |
Where? |
When? |
|
|
|
|
|
|
|
Been sued for nonpayment of rent? |
|
|
|
|
If yes, Who? |
Where? |
When? |
|
|
|
|
|
|
|
Been sued for damage to rental property? |
|
|
|
|
If yes, Who? |
Where? |
When? |
|
|
|
|
|
|
|
Been arrested for criminal activity? |
|
|
|
|
If yes, Who? |
Where? |
When? |
|
|
|
|
|
|
|
Been convicted of a crime? |
|
|
|
|
If yes, Who? |
Where? |
When? |
|
|
|
|
|
||
Been arrested and/or convicted for the use, sale, manufacture, or distribution of any controlled substance? |
|
|
||
If yes, Who? |
Where? |
When? |
|
|
|
|
|
|
|
Lived in Subsidized Housing (Public Housing, Section 8, etc.)? |
|
|
|
|
If yes, Who? |
Where? |
When? |
|
|
|
|
|
||
Been evicted from Public or Assisted housing for violent criminal or drug related activity? |
|
|
||
If yes, Who? |
Where? |
When? |
|
|
|
|
|
|
|
Used a name other than the one you are using now? |
|
|
|
|
If yes, what name? |
|
|
|
|
|
|
|
|
|
Used a social security number other than the one listed above? |
|
|
|
|
If yes, what is it? |
|
|
|
|
|
|
|
||
|
|
|
||
DO YOU, YOUR SPOUSE, OR ANY HOUSEHOLD MEMBERS LISTED ON YOUR APPLICATION: |
YES |
NO |
||
|
|
|
|
|
|
|
|
|
|
Currently use a controlled substance or illegal drug? |
|
|
|
|
If yes, explain |
|
|
|
|
|
|
|
|
|
Owe money to a Public or Assisted Housing Agency? |
|
|
|
|
If yes, Who? |
What Agency? |
|
|
|
Have any relatives (by blood or marriage) who are now an employee of Waco Housing Authority?
If yes, Who?
Are you or anyone listed on your application a registered sex offender?
Does anyone listed on page 1 as a “Household Member” claim mobility, visual or hearing impairment, or other special need which would require a special type of unit or other accommodation?
If yes, please describe:
Do you expect anyone to move in or out of your household within the next 12 months?
If yes, explain:
Does anyone live with you now that is not listed on page 1?
If yes, who?
Do you have any pets?
If yes, what kind?
5