
It is possible to complete jw dpa card easily with our online tool for PDF editing. In order to make our editor better and easier to work with, we consistently design new features, with our users' suggestions in mind. By taking a couple of simple steps, you may start your PDF journey:
Step 1: Click the "Get Form" button in the top part of this webpage to get into our PDF editor.
Step 2: With the help of our online PDF file editor, you may accomplish more than just complete blanks. Try all the functions and make your docs seem high-quality with customized text put in, or optimize the file's original input to excellence - all that backed up by the capability to add any type of graphics and sign the document off.
This PDF will need specific information to be filled in, hence ensure that you take whatever time to enter precisely what is asked:
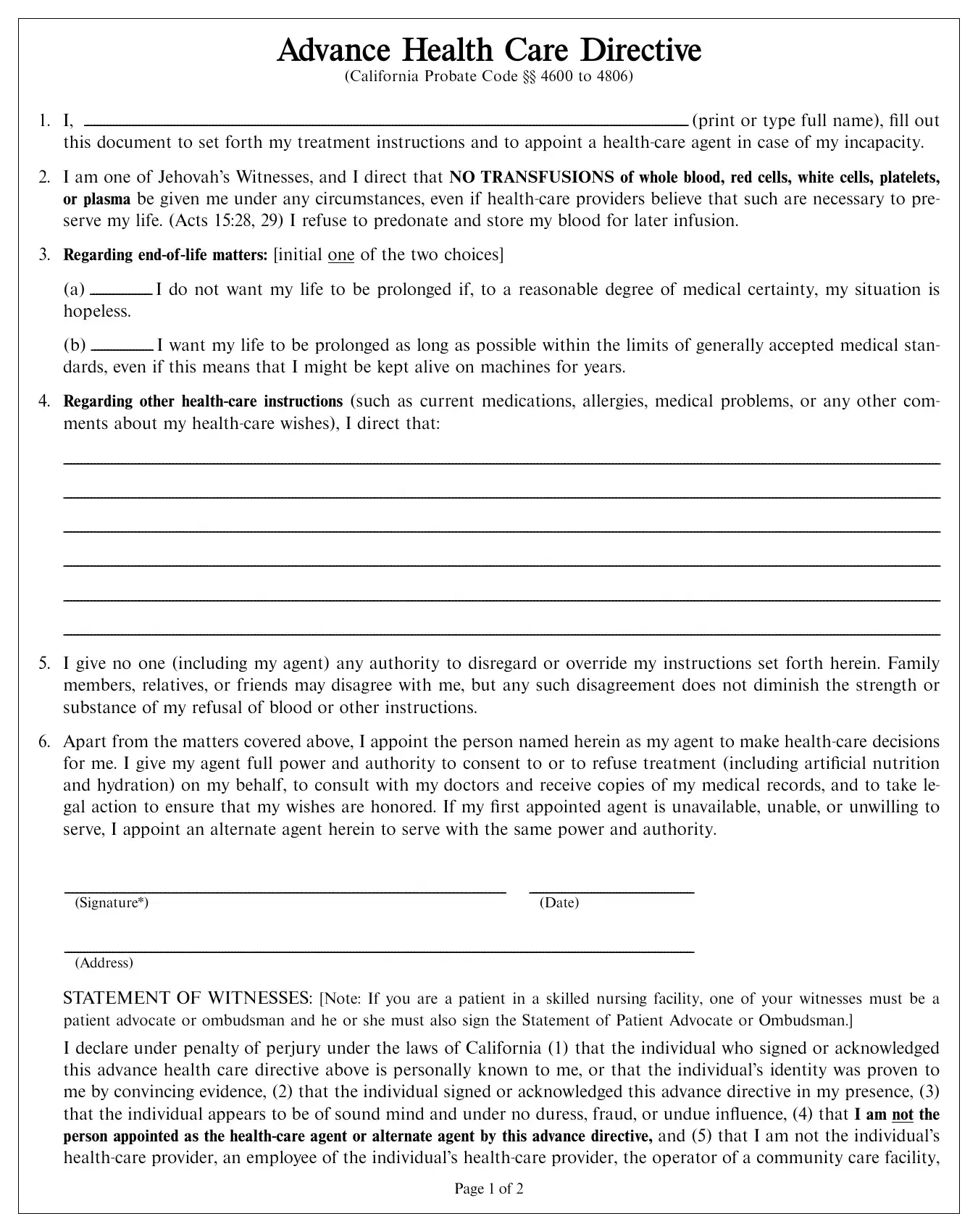
1. It is recommended to fill out the jw dpa card properly, so take care while working with the sections comprising these fields:
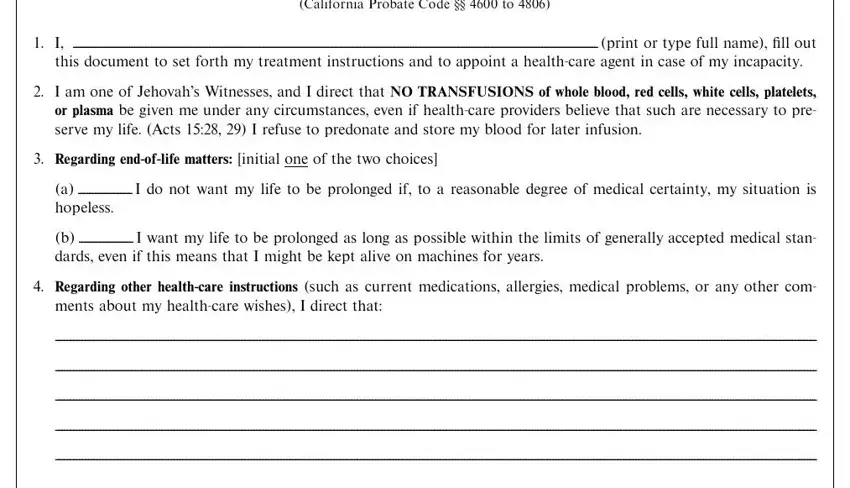
2. Once your current task is complete, take the next step – fill out all of these fields - Apart from the matters covered, Signature, Date, Address, STATEMENT OF WITNESSES Note If you, I declare under penalty of perjury, and Page of with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
3. Within this step, look at an employee of an operator of a, Signature of witness Date, Signature of witness Date, Address, Address, ADDITIONAL STATEMENT OF WITNESSES, I further declare under penalty of, Signature, Signature, SPECIAL WITNESS REQUIREMENT If you, STATEMENT OF PATIENT ADVOCATE OR, and I declare under penalty of perjury. Each one of these should be taken care of with utmost accuracy.
When it comes to I further declare under penalty of and SPECIAL WITNESS REQUIREMENT If you, be sure that you double-check them in this section. These two are definitely the key ones in this file.
4. This next section requires some additional information. Ensure you complete all the necessary fields - HEALTHCARE AGENT, Name, Address, Telephones, Note Before signing this document, ALTERNATE HEALTHCARE AGENT, Advance Health Care Directive, Name, Address, Telephones, dpaE Uca, Page of, signed document inside, and NO BLOOD - to proceed further in your process!
Step 3: Reread all the information you've typed into the form fields and click the "Done" button. Sign up with FormsPal today and immediately obtain jw dpa card, set for downloading. Each and every modification you make is conveniently preserved , helping you to modify the file at a later time anytime. FormsPal guarantees secure document tools with no personal data record-keeping or distributing. Rest assured that your information is in good hands here!