Form CMS-1763, also known as “Request for Termination of Premium Hospital and/or Supplementary Medical Insurance,” is used by individuals who wish to voluntarily terminate their Medicare Part A (hospital insurance) and/or Medicare Part B (medical insurance). This form is crucial for those who, for various reasons, decide that they no longer want to continue their coverage under these parts of Medicare. The termination of Medicare benefits is a significant decision that requires the completion and submission of CMS-1763 to ensure that the request is processed correctly and that the individual understands the implications of terminating their Medicare coverage.
The process for using CMS-1763 involves contacting the Social Security Administration (SSA) to set up an interview, during which the form is completed. This interview can be conducted either in person at an SSA office or over the phone. The purpose of the interview and the form is to ensure that the individual fully understands the consequences of discontinuing their Medicare coverage, such as potential gaps in health insurance and the need for alternative coverage.
Other CMS Forms
Take a look at a few other CMS PDFs accessible for editing with our editor. Besides that, remember that you can actually upload, fill out, and edit any PDF form at FormsPal.
You will need to provide an original signature, while other sections of this paper might be completed electronically. To obtain a customized PDF document, we suggest you use our form-building software.
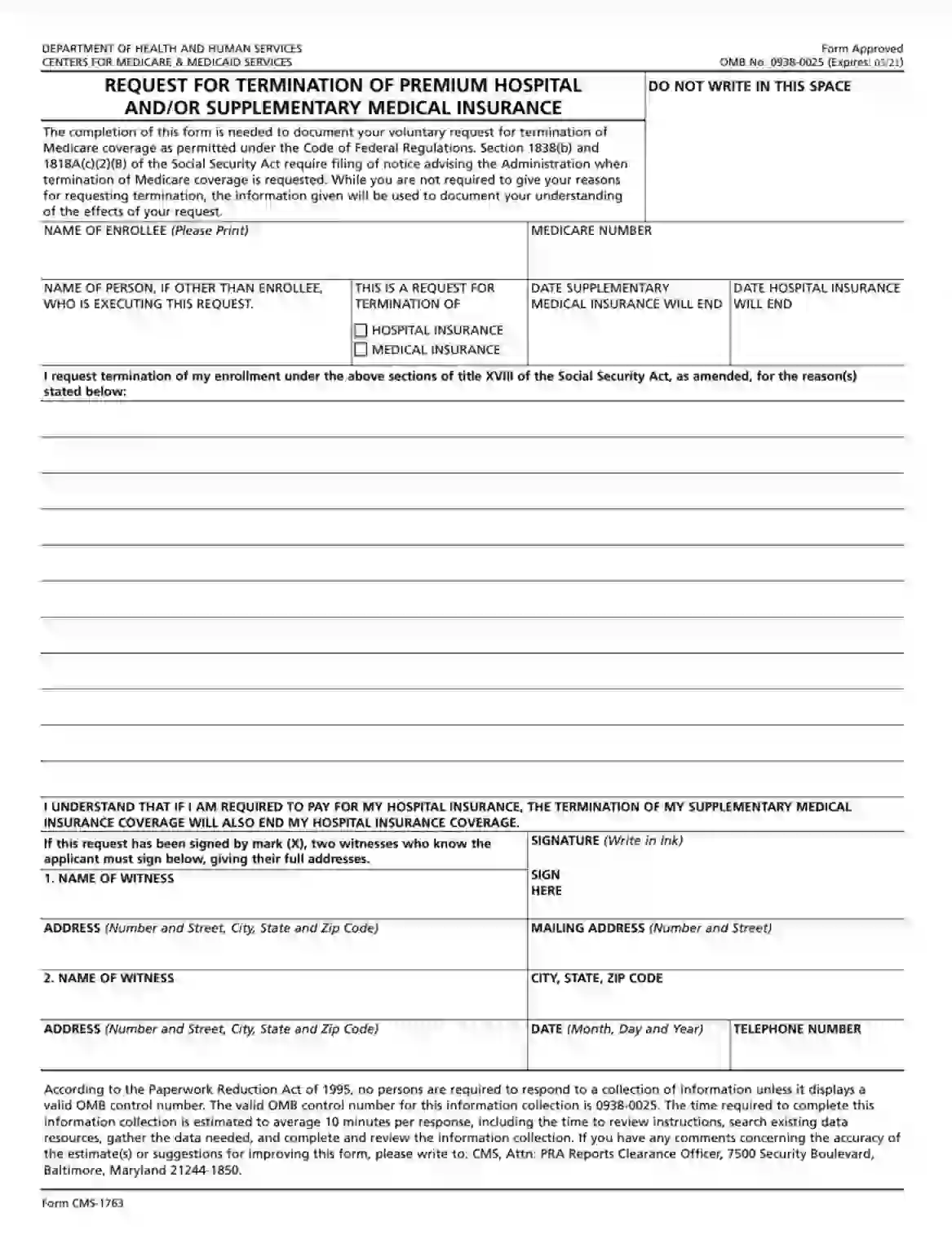
A full name (including your middle initial) has to be printed (or put in handwriting) herein.

Each enrollee possesses a personal Medicare number that allows the Department of Health and Human Services to identify them. Input yours in this box.

If you have decided to complete this paper with the assistance of a designated attorney or legal representative of the enrollee, please indicate their name.

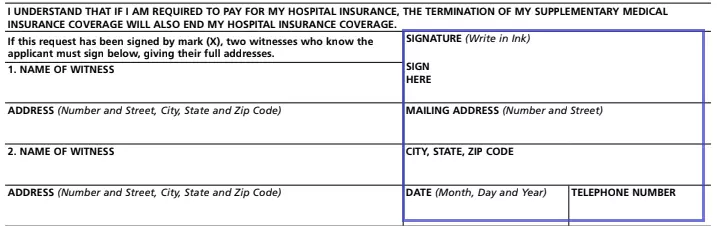
You may choose to terminate hospital insurance, medical insurance, or both. Check the corresponding box.
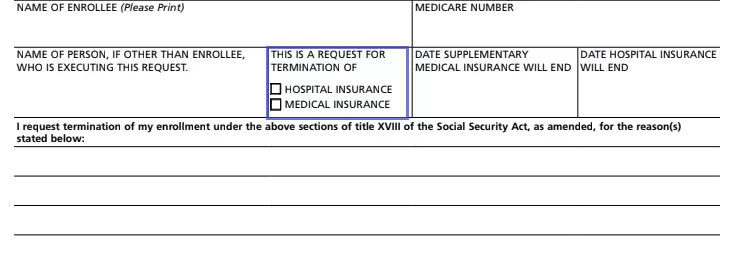
An enrollee has to insert the date when they expect their insurance to end.

The CMS and SSA need to understand why exactly you have opted for terminating Medicare coverage. So, if that is your case, make sure to provide lawful reasoning.
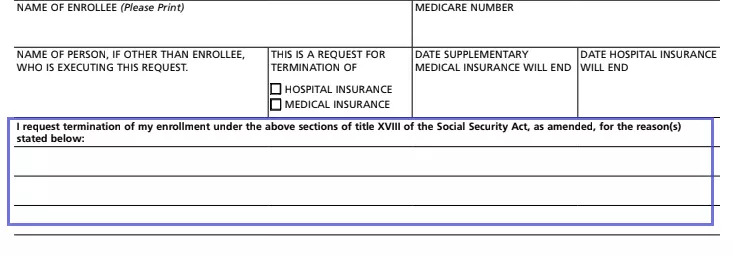
Review the data you have submitted and append your signature. Write in ink. Do not forget to insert your complete residential address (including house number, street, city, state, and zip code), the date you are signing the paper on, and a phone number below.
In case an enrollee has signed the form with an “X,” this document will not be considered effective unless witnessed by two competent adults. They must provide their full names, along with the mailing addresses (including house number, street, city, state, and zip code).