Here’s a guide on how to fill out the Alaska Motor Vehicle Crash Form 12-209, ensuring that all required details are properly documented.
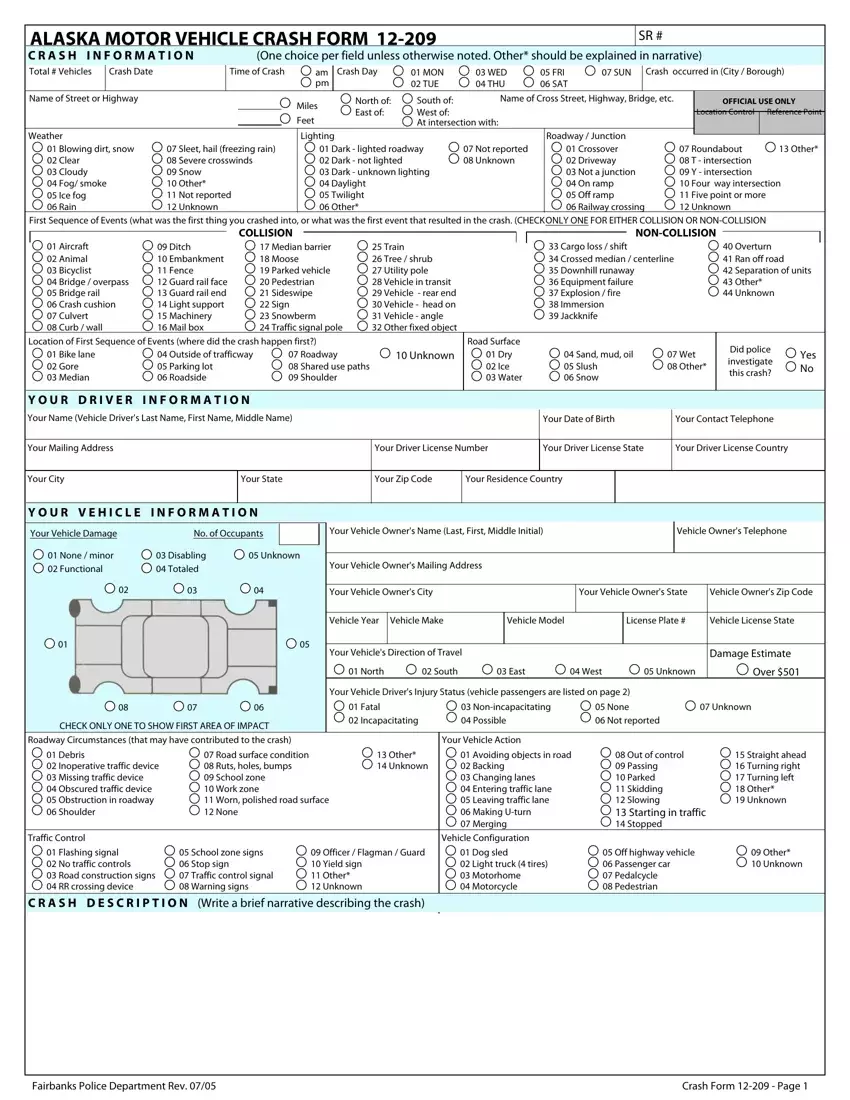
1. Document Basic Crash Information
Start by filling in the SR number and total number of vehicles involved. Specify the crash date, time, and day of the week. Select the applicable weather condition from the provided options. If the condition is not listed, select "Other" and describe it in the narrative section later.
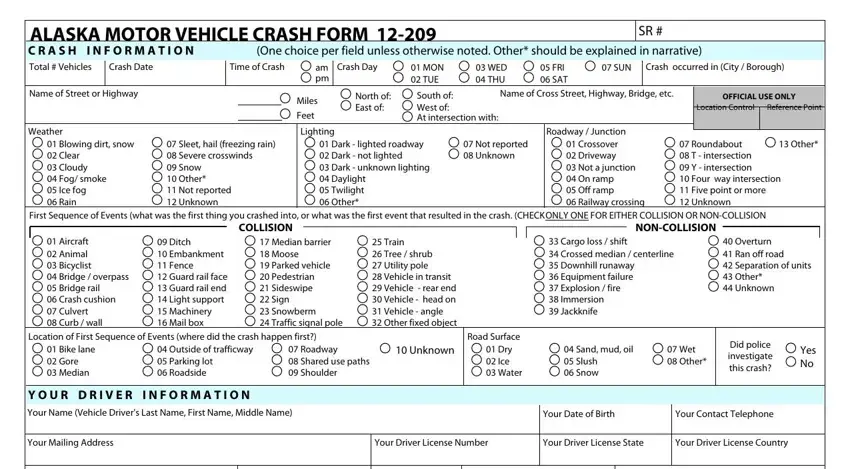
2. Specify the Location and First Sequence of Events
Indicate the name of the street or highway where the crash occurred. For the first sequence of events, check only one box that best describes the initial impact or event leading to the crash. Specify the exact location of this event using the provided location options.
3. Enter Your Driver Information
Provide your full name, mailing address, city, state, zip code, driver's license number, and the country and state where your license was issued. Include your date of birth and contact telephone number. Specify the city or borough where the crash occurred.
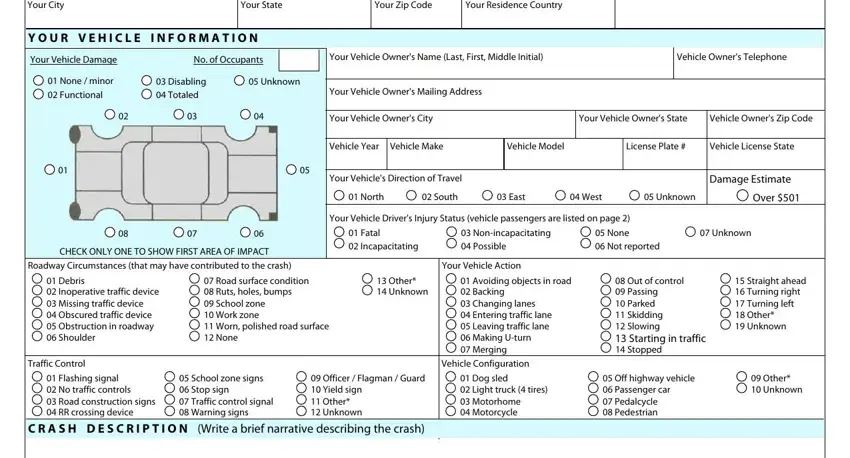
4. Describe Your Vehicle Information
Detail your vehicle’s make, model, year, and license plate number. Indicate the vehicle’s direction of travel at the time of the crash. Document the first area of impact on your vehicle and the estimated damage in monetary terms.
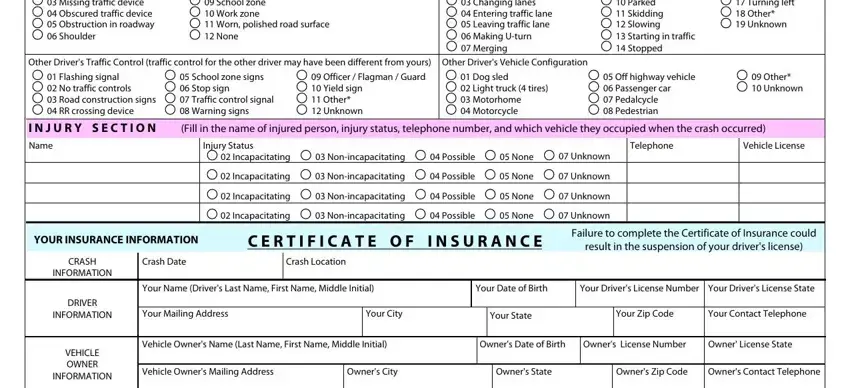
5. Report Insurance Information
State whether there was an active automobile liability policy covering the accident. Include the insurance company's name, your policy number, and the insurance agent's contact information. Confirm the validity period of the insurance policy.
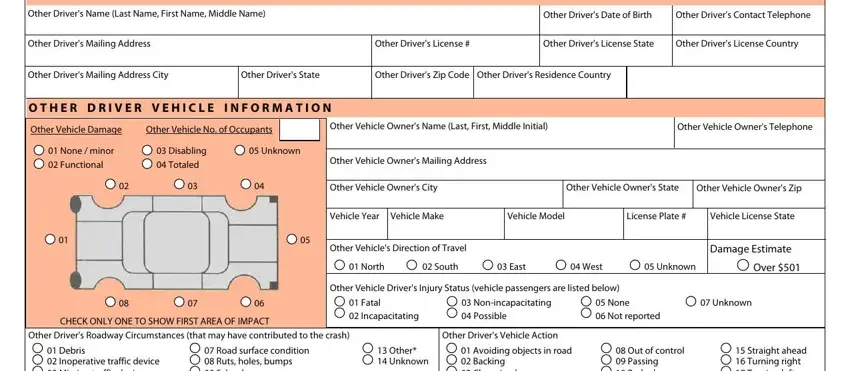
6. Provide Vehicle Owner Information
If you are not the vehicle owner, enter the vehicle owner's name, mailing address, contact information, and any additional relevant details. Specify the owner's relationship to the vehicle if it's not self-owned.
7. Record Detailed Crash and Damage Description
Use the crash description section to write a brief narrative of how the crash occurred, including any significant details that the form has not already covered. Be clear and concise, focusing on the sequence of events and any contributing factors.
8. List Injuries and Other Damages
If applicable, provide information about any injuries resulting from the crash. Include the injured person's name, extent of their injuries, contact information, and vehicle they occupied during the crash.
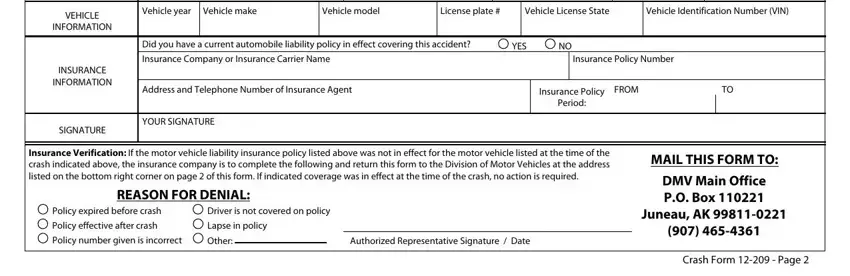
9. Sign and Date the Form
Sign and date the form after reviewing all the information for accuracy and completeness. Ensure that all mandatory fields are filled to avoid issues with processing.
10. Submit the Completed Form
Finally, mail the completed form to the appropriate department as indicated on the form. Make sure to keep a copy for your records.
