
FRONTAGE can be completed online very easily. Just try FormsPal PDF tool to accomplish the job right away. FormsPal is dedicated to providing you with the absolute best experience with our editor by constantly introducing new features and improvements. With all of these updates, working with our editor becomes easier than ever! Here is what you'll want to do to start:
Step 1: Click on the orange "Get Form" button above. It's going to open up our editor so that you could start filling out your form.
Step 2: The editor will allow you to modify your PDF file in many different ways. Enhance it by writing personalized text, correct existing content, and place in a signature - all at your convenience!
It really is simple to finish the pdf using this detailed tutorial! Here's what you should do:
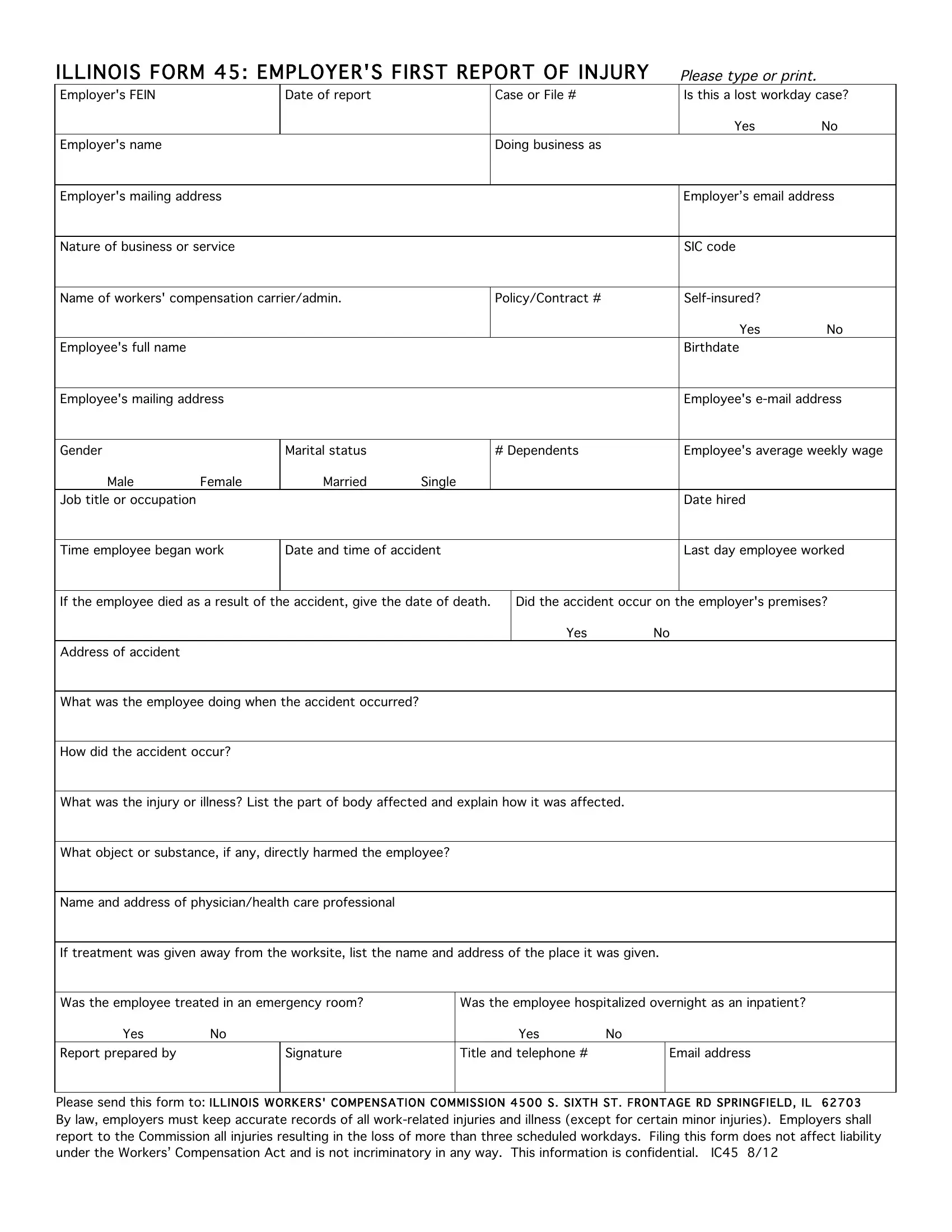
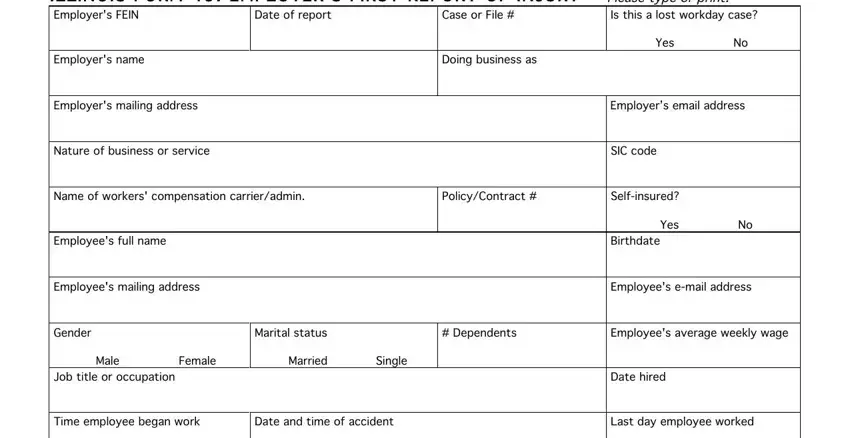
1. Whenever submitting the FRONTAGE, be sure to include all essential blank fields in its associated form section. This will help expedite the work, allowing for your information to be handled quickly and properly.
2. Once your current task is complete, take the next step – fill out all of these fields - If the employee died as a result, Address of accident, What was the employee doing when, How did the accident occur, Did the accident occur on the, Yes No, What was the injury or illness, What object or substance if any, Name and address of, If treatment was given away from, Was the employee treated in an, Was the employee hospitalized, Yes No Report prepared by, Signature, and Yes No Title and telephone with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
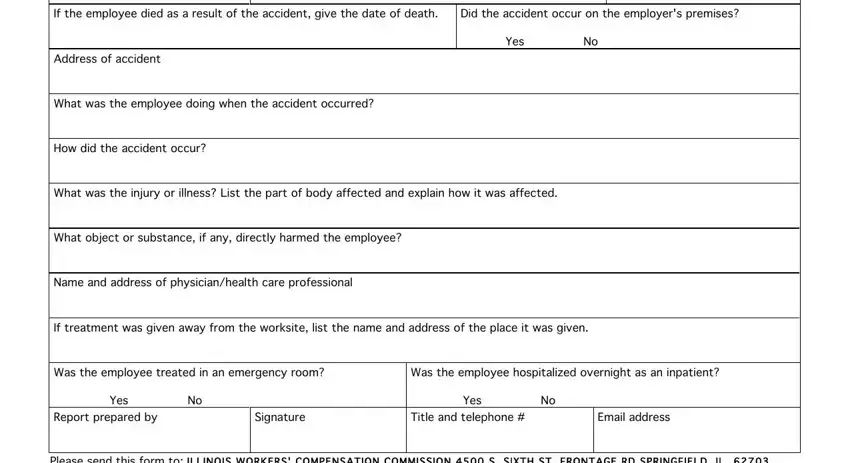
Always be very careful when completing Did the accident occur on the and How did the accident occur, as this is where most people make a few mistakes.
Step 3: Make sure that the details are correct and then click on "Done" to complete the task. Sign up with us right now and easily get FRONTAGE, all set for downloading. Each and every modification made is handily preserved , which enables you to customize the file later when necessary. FormsPal is invested in the privacy of all our users; we always make sure that all personal data used in our editor remains protected.