

In case you desire to fill out osha's form 300a, you won't have to download and install any applications - simply give a try to our PDF tool. To have our tool on the cutting edge of efficiency, we strive to implement user-driven capabilities and enhancements on a regular basis. We are always looking for suggestions - join us in revolutionizing how you work with PDF documents. With some basic steps, you can begin your PDF journey:
Step 1: Simply press the "Get Form Button" above on this site to see our pdf editing tool. There you'll find everything that is needed to fill out your file.
Step 2: With this advanced PDF file editor, it is possible to do more than just fill out forms. Try each of the functions and make your forms appear sublime with customized text put in, or optimize the file's original content to perfection - all accompanied by an ability to insert your personal graphics and sign it off.
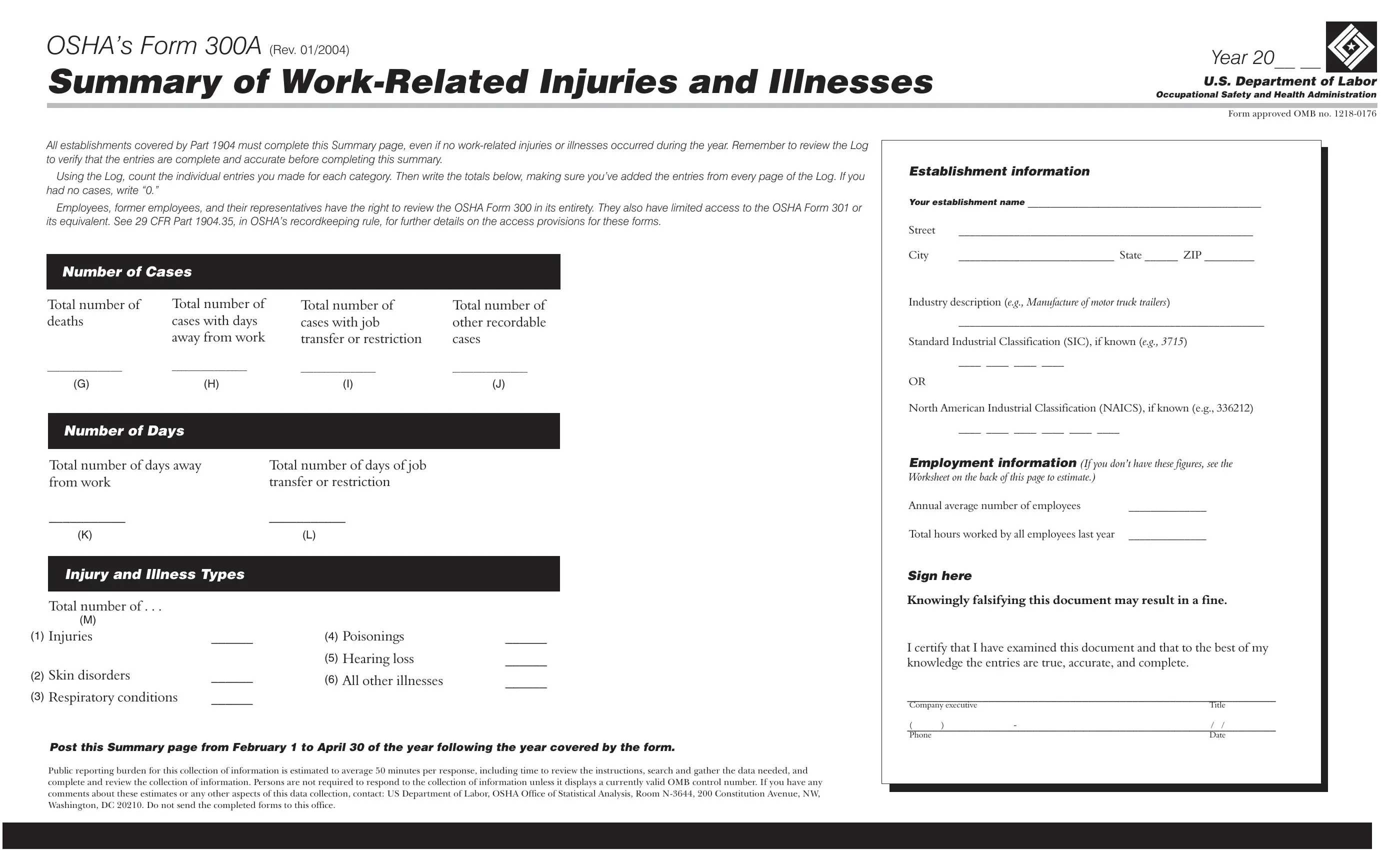
For you to complete this form, be sure you enter the necessary details in each and every field:
1. Whenever submitting the osha's form 300a, make sure to complete all important blank fields within its corresponding form section. It will help facilitate the process, which allows your details to be handled efficiently and correctly.
2. Right after this section is done, proceed to type in the relevant details in all these - K L, Injury and Illness Types, Total number of , M Injuries, Skin disorders, Respiratory conditions, Poisonings, Hearing loss, All other illnesses, Post this Summary page from, Public reporting burden for this, Annual average number of employees, Total hours worked by all, Sign here, and Knowingly falsifying this document.
Regarding All other illnesses and Public reporting burden for this, make sure you get them right in this section. Both of these could be the most significant ones in the form.
Step 3: Check what you've entered into the form fields and then click the "Done" button. Make a 7-day free trial plan at FormsPal and obtain immediate access to osha's form 300a - download or edit inside your FormsPal cabinet. FormsPal offers protected form completion without personal information recording or any sort of sharing. Feel safe knowing that your data is safe with us!