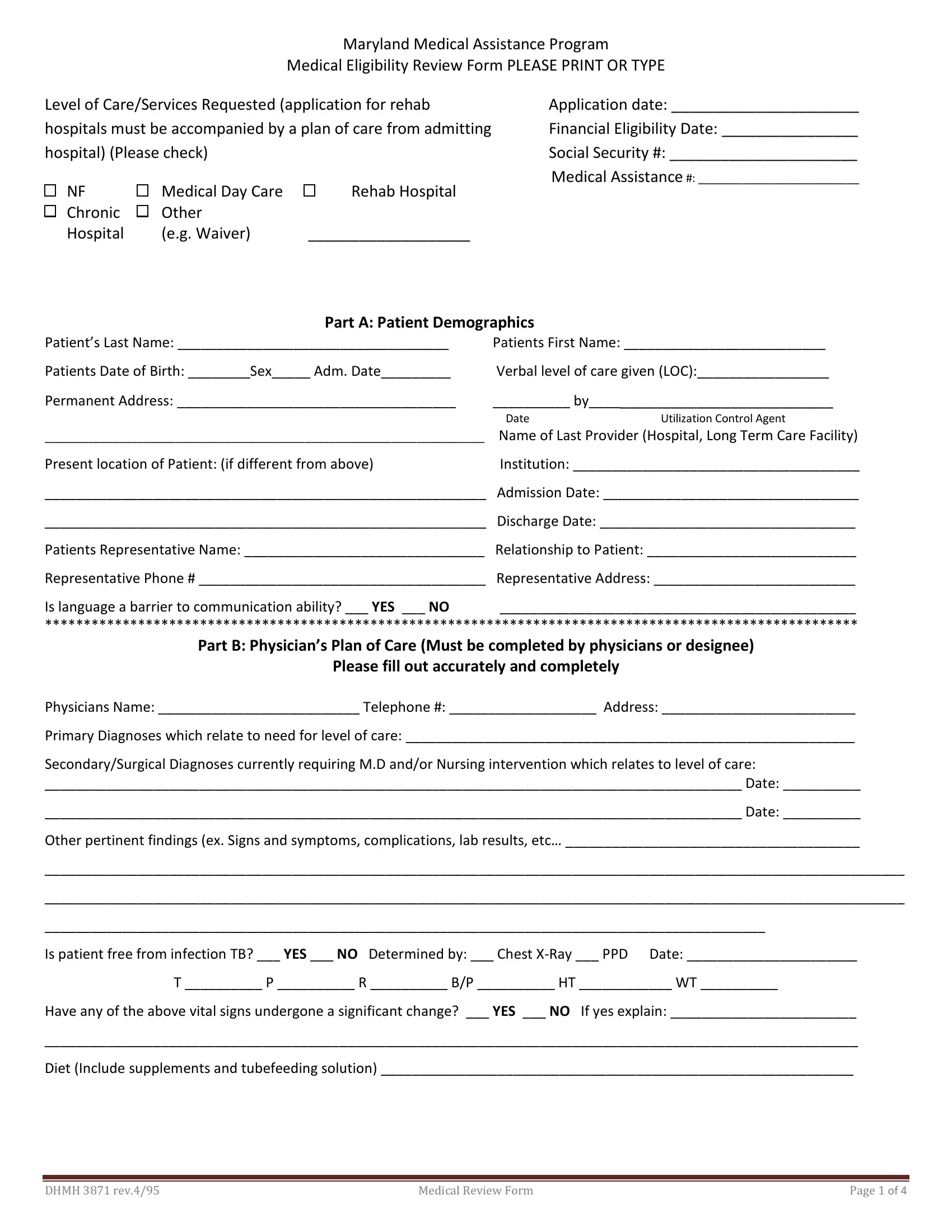
The 3871 Maryland Medicaid form serves as a critical component in the process of determining medical eligibility for individuals seeking assistance through the Maryland Medical Assistance Program. This comprehensive form not only requests detailed demographic information about patients but also requires a precise outline of the level of care or services needed, underscored by the necessity of a plan of care from the admitting hospital for applicants aiming for rehabilitation services. Key sections cover financial eligibility, patient demographics, physician’s plans of care, and assessments of the patient's functional, cognitive, and behavioral status, concluding with a segment dedicated to physician certification for the required level of care. With fields that demand information ranging from basic identification details, such as Social Security and Medical Assistance numbers, to more intricate descriptions of the patient’s medical and functional conditions, treatments to be continued, and an active therapy plan, it underscores the thorough evaluation process adopted by the Maryland Medical Assistance Program to ensure that applicants receive the appropriate level of care. Moreover, the form includes sections that cater to different age groups and addresses specific needs, reflecting an understanding of the diverse population the program serves. This intricate document facilitates a structured pathway for healthcare providers and applicants to convey critical information, supporting the process of establishing medical eligibility and furthering access to much-needed healthcare services.
| Question | Answer |
|---|---|
| Form Name | 3871 Maryland Medicaid Form |
| Form Length | 4 pages |
| Fillable? | Yes |
| Fillable fields | 217 |
| Avg. time to fill out | 22 min 14 sec |
| Other names | 3871 maryland medicaud, form 3871 maryland, 3871 form medically, 3871 maryland form |
