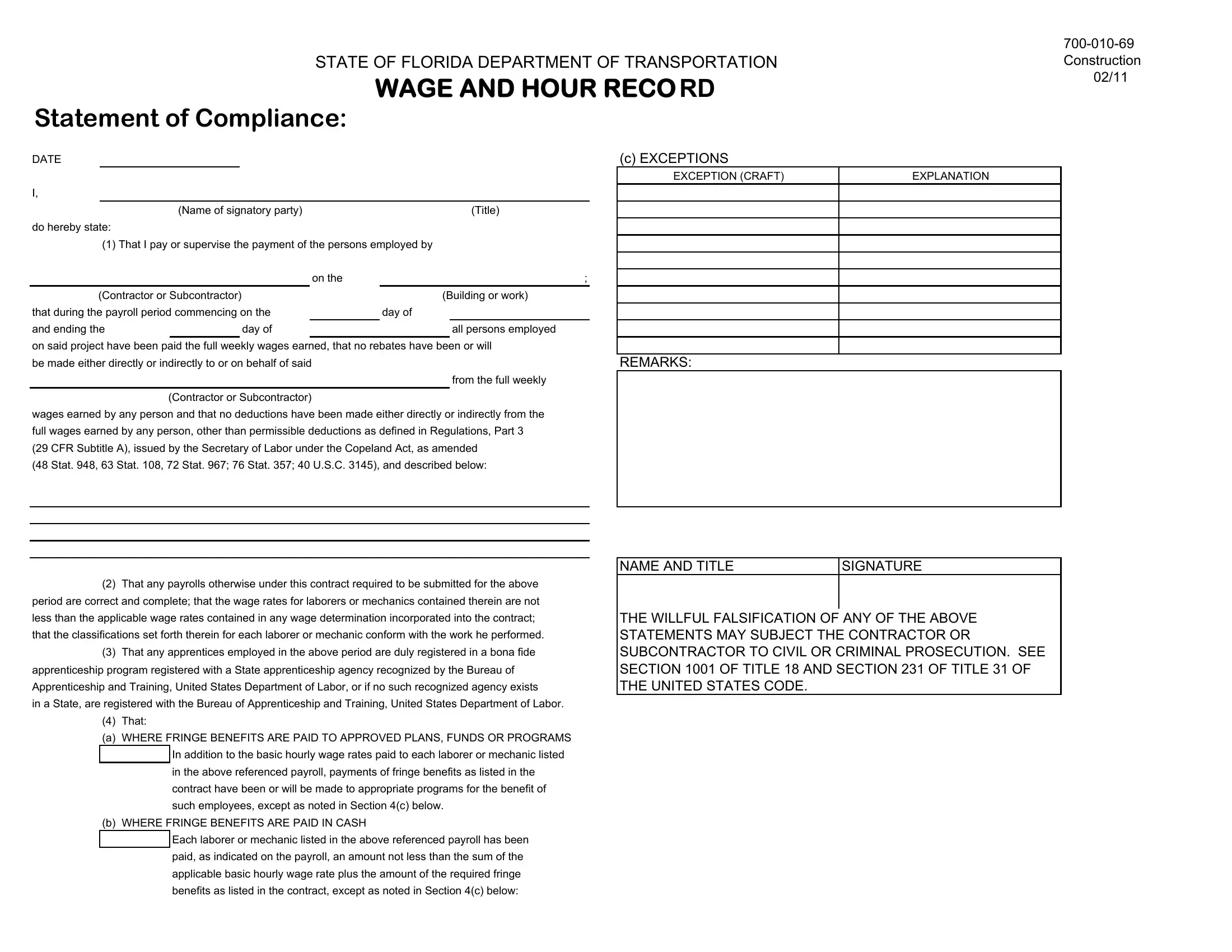
The 700 010 69 form, issued by the State of Florida Department of Transportation, serves a pivotal role in ensuring fair wage practices within the framework of construction projects. This comprehensive document, encompassing a statement of compliance, wage and hour record, deductions record, and fringe benefits record, mandates a declaration by signatories that all employees have received their rightfully earned wages, without improper deductions or rebates, during a specified payroll period. It further requires the assurance that payroll submissions are accurate and adhere to the minimum wage rates as per contract stipulations and that any employed apprentices are registered with recognized apprenticeship programs. Moreover, the form details the provision of fringe benefits, whether paid into approved plans or directly in cash, highlighting a commitment to upholding employee rights and labor standards. The responsibility placed on contractors or subcontractors to accurately report hourly wages, deductions, and fringe benefits underscores the form’s critical role in protecting laborers and mechanics from wage theft and promoting transparency. Notably, the document warns that falsification of these statements could lead to civil or criminal prosecution, underscoring the legal seriousness of the form's assertions.
| Question | Answer |
|---|---|
| Form Name | 700 010 69 Form |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | fdot form 275 010 69, 700 69 fdot form, 700 010 fdot form, 700 010 69 |
STATE OF FLORIDA DEPARTMENT OF TRANSPORTATION
WAGE AND HOUR RECO RD
Statement of Compliance:
DATE
I,
|
(Name of signatory party) |
|
|
|
(Title) |
|||
do hereby state: |
|
|
|
|
|
|
|
|
(1) That I pay or supervise the payment of the persons employed by |
||||||||
|
|
|
|
on the |
; |
|||
(Contractor or Subcontractor) |
|
(Building or work) |
||||||
that during the payroll period commencing on the |
|
|
day of |
|
||||
and ending the |
|
day of |
|
|
|
|
all persons employed |
|
on said project have been paid the full weekly wages earned, that no rebates have been or will be made either directly or indirectly to or on behalf of said
from the full weekly
(Contractor or Subcontractor)
wages earned by any person and that no deductions have been made either directly or indirectly from the full wages earned by any person, other than permissible deductions as defined in Regulations, Part 3 (29 CFR Subtitle A), issued by the Secretary of Labor under the Copeland Act, as amended
(48 Stat. 948, 63 Stat. 108, 72 Stat. 967; 76 Stat. 357; 40 U.S.C. 3145), and described below:
(c) EXCEPTIONS
EXCEPTION (CRAFT) |
EXPLANATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
REMARKS:
(2)That any payrolls otherwise under this contract required to be submitted for the above period are correct and complete; that the wage rates for laborers or mechanics contained therein are not less than the applicable wage rates contained in any wage determination incorporated into the contract; that the classifications set forth therein for each laborer or mechanic conform with the work he performed.
(3)That any apprentices employed in the above period are duly registered in a bona fide apprenticeship program registered with a State apprenticeship agency recognized by the Bureau of Apprenticeship and Training, United States Department of Labor, or if no such recognized agency exists
in a State, are registered with the Bureau of Apprenticeship and Training, United States Department of Labor.
(4)That:
(a) WHERE FRINGE BENEFITS ARE PAID TO APPROVED PLANS, FUNDS OR PROGRAMS In addition to the basic hourly wage rates paid to each laborer or mechanic listed in the above referenced payroll, payments of fringe benefits as listed in the contract have been or will be made to appropriate programs for the benefit of such employees, except as noted in Section 4(c) below.
(b) WHERE FRINGE BENEFITS ARE PAID IN CASH
Each laborer or mechanic listed in the above referenced payroll has been paid, as indicated on the payroll, an amount not less than the sum of the applicable basic hourly wage rate plus the amount of the required fringe benefits as listed in the contract, except as noted in Section 4(c) below:
NAME AND TITLE |
SIGNATURE |
|
|
THE WILLFUL FALSIFICATION OF ANY OF THE ABOVE STATEMENTS MAY SUBJECT THE CONTRACTOR OR SUBCONTRACTOR TO CIVIL OR CRIMINAL PROSECUTION. SEE SECTION 1001 OF TITLE 18 AND SECTION 231 OF TITLE 31 OF THE UNITED STATES CODE.
Wage and Hour Record:
Contractor's Name
Payroll Number:
(1) |
|
|
Employee Name |
|
|
and 4 Digit Identifier |
|
|
(9 digit SS and full address |
(2) |
|
required on contracts Let |
||
Exemptions / |
||
prior to 1/19/09) |
||
Race & |
||
|
||
|
Gender |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Construction |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
02/11 |
|
|
|
|
|
|
|
|
|
|
|
|
Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
Contract # |
|
|
|
|
|
Project and Location |
|
|
|
|
|
|
||
For Week Ending |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
FIN # |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(4) |
Day and Date |
|
(6) |
|
(7) |
|
(8) |
Deductions |
|
(9) |
|
|
(10) |
|
||||||||
|
|
(5) |
|
|
|
|
|
|
||||||||||||||||
|
|
Total |
Pay Rate |
|
Project |
|
|
Net Wages |
|
Total from |
|
|||||||||||||
|
|
|
|
|
|
|
|
|
Hours |
|
|
Gross / |
FICA |
With- |
|
|
|
Total from |
Total |
Paid for |
|
Fringe Benefit |
|
|
|
Time |
|
|
|
|
|
|
|
|
|
|
Weekly |
|
holding |
|
|
|
Deduction |
Deductions |
|
|
|||
(3) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
week |
|
|
Sheet |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
Over |
|
|
|
|
|
|
|
|
|
|
Gross |
|
tax |
|
|
|
Sheet |
|
|
|
|
(attached) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Work Classif- |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(attached) |
|
|
|
|
|
|
ication |
Stright |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
O |
|
|
|
|
|
|
|
0.00 |
0.00 |
|
0.00 |
|
|
|
|
|
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
0.00 |
|
|
|
|
|
|
|
|
|
$0.00 |
$ |
- |
|
|
|
|
O |
|
|
|
|
|
|
|
0.00 |
0.00 |
|
0.00 |
|
|
|
|
|
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
0.00 |
|
|
|
|
|
|
|
|
|
$0.00 |
$ |
- |
|
|
|
|
O |
|
|
|
|
|
|
|
0.00 |
0.00 |
|
0.00 |
|
|
|
|
|
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
0.00 |
|
|
|
|
|
|
|
|
|
$0.00 |
$ |
- |
|
|
|
|
O |
|
|
|
|
|
|
|
0.00 |
0.00 |
|
0.00 |
|
|
|
|
|
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
0.00 |
|
|
|
|
|
|
|
|
|
$0.00 |
$ |
- |
|
|
|
|
O |
|
|
|
|
|
|
|
0.00 |
0.00 |
|
0.00 |
|
|
|
|
|
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
0.00 |
|
|
|
|
|
|
|
|
|
$0.00 |
$ |
- |
|
|
|
|
O |
|
|
|
|
|
|
|
0.00 |
0.00 |
|
0.00 |
|
|
|
|
|
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
0.00 |
|
|
|
|
|
|
|
|
|
$0.00 |
$ |
- |
|
|
|
|
O |
|
|
|
|
|
|
|
0.00 |
0.00 |
|
0.00 |
|
|
|
|
|
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
0.00 |
|
|
|
|
|
|
|
|
|
$0.00 |
$ |
- |
|
|
|
|
O |
|
|
|
|
|
|
|
0.00 |
0.00 |
|
0.00 |
|
|
|
|
|
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
0.00 |
|
|
|
|
|
|
|
|
|
$0.00 |
$ |
- |
|
|
|
|
O |
|
|
|
|
|
|
|
0.00 |
0.00 |
|
0.00 |
|
|
|
|
|
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
0.00 |
|
|
|
|
|
|
|
|
|
$0.00 |
$ |
- |
|
|
|
|
O |
|
|
|
|
|
|
|
0.00 |
0.00 |
|
0.00 |
|
|
|
|
|
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
0.00 |
|
|
|
|
|
|
|
|
|
$0.00 |
$ |
- |
|
|
|
|
O |
|
|
|
|
|
|
|
0.00 |
0.00 |
|
0.00 |
|
|
|
|
|
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
0.00 |
|
|
|
|
|
|
|
|
|
$0.00 |
$ |
- |
|
|
|

Deductions Record:
Contractor's Name
Payroll Number:
Address
For Week Ending
FIN #
Contract #
Project and Location
|
|
Type a Deduction description in each box and then record the amount of that Deduction for each employee (or leave blank). |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
Employee Name (last, first) |
|
|
|
|
|
|
|
|
|
|
Total |
|
|
|
|
|
|
|
|
|
|
Deductions |
|
|
|
|
|
|
|
|
|
|
|
|
Amount |
|
|
|
|
|
|
|
|
|
|
|
$0.00 |
|
|
|
|
|
|
|
|
|
|
|
$0.00 |
|
|
|
|
|
|
|
|
|
|
|
$0.00 |
|
|
|
|
|
|
|
|
|
|
|
$0.00 |
|
|
|
|
|
|
|
|
|
|
|
$0.00 |
|
|
|
|
|
|
|
|
|
|
|
$0.00 |
|
|
|
|
|
|
|
|
|
|
|
$0.00 |
|
|
|
|
|
|
|
|
|
|
|
$0.00 |
|
|
|
|
|
|
|
|
|
|
|
$0.00 |
|
|
|
|
|
|
|
|
|
|
|
$0.00 |
|
|
|
|
|
|
|
|
|
|
|
$0.00 |
|
|
|
|
|
|
|
|
|
|
|
$0.00 |
|
|
|
|
|
|
|
|
|
|
|
$0.00 |
|
|
|
|
|
|
|
|
|
|
|
$0.00 |
|
|
|
|
|
|
|
|
|
|
|
$0.00 |
|
|
|
|
|
|
|
|
|
|
|
$0.00 |
|
|
|
|
|
|
|
|
|
|
|
$0.00 |
|
|
|
|
|
|
|
|
|
|
|
$0.00 |
|
|
|
|
|
|
|
|
|
|
|
$0.00 |
|
|
|
|
|
|
|
|
|
|
|
$0.00 |
|
|
|
|
|
|
|
|
|
|
|
$0.00 |
|
|
|
|
|
|
|
|
|
|
|
$0.00 |
|
|
|
|
|
|
|
|
|
|
|
$0.00 |
Fringe Benefits Record:
Contractor's Name
Payroll Number: |
|
For Week Ending |
FIN #
Address
Contract #
Project and Location
Type a Fringe Benefit description in each box and then record the amount of that Fringe for each employee (or leave blank).
Employee Name (last, first)
Total
Fringe
Benefit
Amount
$0.00
$0.00
$0.00
$0.00
$0.00
$0.00
$0.00
$0.00
$0.00
$0.00
$0.00
$0.00
$0.00
$0.00
$0.00
$0.00
$0.00
$0.00
$0.00
$0.00
$0.00
$0.00