ABA concurrent form is a type of ABA therapy that uses two therapists to work with a child simultaneously. The therapist who is working with the child on their functional goals, or "target" tasks, is called the "active" therapist. The therapist who is providing support and prompting for the active therapist is called the "support" therapist. This type of therapy can be used in a variety of settings, including home, school, and clinic settings. ABA concurrent form has been found to be an effective treatment for many children with ASD and other developmental disabilities.
| Question | Answer |
|---|---|
| Form Name | Aba Concurrent Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | na treatment aba, applied behavioral analysis concurrent, behavioral concurrent online, applied behavioral report |

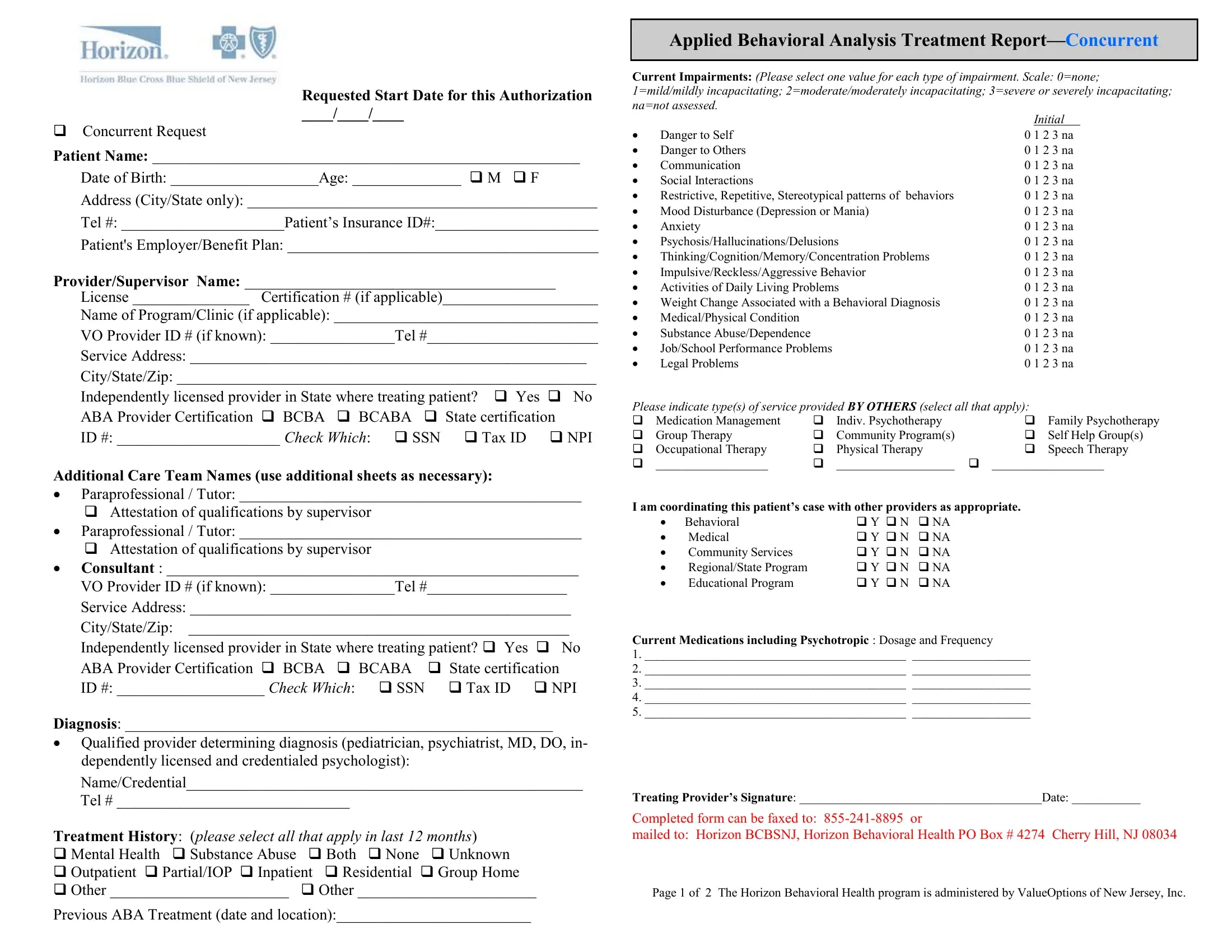
Requested Start Date for this Authorization
____/____/____
Concurrent Request
Patient Name: _______________________________________________________
Date of Birth: ___________________Age: ______________ M F
Address (City/State only): _____________________________________________
Tel #: _____________________Patient’s Insurance ID#:_____________________
Patient's Employer/Benefit Plan: ________________________________________
Provider/Supervisor Name: ________________________________________
License _______________ Certification # (if applicable)____________________
Name of Program/Clinic (if applicable): __________________________________
VO Provider ID # (if known): ________________Tel #______________________
Service Address: ___________________________________________________
City/State/Zip: ______________________________________________________
Independently licensed provider in State where treating patient? Yes No ABA Provider Certification BCBA BCABA State certification
ID #: _____________________ Check Which: SSN Tax ID NPI
Additional Care Team Names (use additional sheets as necessary):
∙Paraprofessional / Tutor: ____________________________________________
Attestation of qualifications by supervisor
∙Paraprofessional / Tutor: ____________________________________________
Attestation of qualifications by supervisor
∙Consultant : _____________________________________________________
VO Provider ID # (if known): ________________Tel #__________________
Service Address: _________________________________________________
City/State/Zip: _________________________________________________
Independently licensed provider in State where treating patient? Yes No
ABA Provider Certification BCBA BCABA |
State certification |
ID #: ___________________ Check Which: SSN |
Tax ID NPI |
Diagnosis: _______________________________________________________
∙Qualified provider determining diagnosis (pediatrician, psychiatrist, MD, DO, in- dependently licensed and credentialed psychologist):
Name/Credential___________________________________________________
Tel # ______________________________
Treatment History: (please select all that apply in last 12 months)
Mental Health Substance Abuse Both None Unknown
Outpatient Partial/IOP Inpatient Residential Group Home
Other _______________________ Other _______________________
Previous ABA Treatment (date and location):_________________________
Applied Behavioral Analysis Treatment
Current Impairments: (Please select one value for each type of impairment. Scale: 0=none; 1=mild/mildly incapacitating; 2=moderate/moderately incapacitating; 3=severe or severely incapacitating; na=not assessed.
|
|
|
|
Initial |
|
∙ |
Danger to Self |
|
0 1 2 3 na |
||
∙ |
Danger to Others |
|
0 1 2 3 na |
||
∙ |
Communication |
|
0 1 2 3 na |
||
∙ |
Social Interactions |
|
0 1 2 3 na |
||
∙ |
Restrictive, Repetitive, Stereotypical patterns of behaviors |
0 1 2 3 na |
|||
∙ |
Mood Disturbance (Depression or Mania) |
0 1 2 3 na |
|||
∙ |
Anxiety |
|
0 1 2 3 na |
||
∙ |
Psychosis/Hallucinations/Delusions |
0 1 2 3 na |
|||
∙ |
Thinking/Cognition/Memory/Concentration Problems |
0 1 2 3 na |
|||
∙ |
Impulsive/Reckless/Aggressive Behavior |
0 1 2 3 na |
|||
∙ |
Activities of Daily Living Problems |
0 1 2 3 na |
|||
∙ |
Weight Change Associated with a Behavioral Diagnosis |
0 1 2 3 na |
|||
∙ |
Medical/Physical Condition |
|
0 1 2 3 na |
||
∙ |
Substance Abuse/Dependence |
|
0 1 2 3 na |
||
∙ |
Job/School Performance Problems |
0 1 2 3 na |
|||
∙ |
Legal Problems |
|
0 1 2 3 na |
||
Please indicate type(s) of service provided BY OTHERS (select all that apply): |
|||||
Medication Management |
Indiv. Psychotherapy |
Family Psychotherapy |
|||
Group Therapy |
Community Program(s) |
Self Help Group(s) |
|||
Occupational Therapy |
Physical Therapy |
Speech Therapy |
|||
__________________ |
___________________ |
__________________ |
|||
I am coordinating this patient’s case with other providers as appropriate.
∙ |
Behavioral |
Y N |
NA |
∙ |
Medical |
Y N |
NA |
∙ |
Community Services |
Y N |
NA |
∙ |
Regional/State Program |
Y N |
NA |
∙ |
Educational Program |
Y N |
NA |
Current Medications including Psychotropic : Dosage and Frequency
1.__________________________________________ ___________________
2.__________________________________________ ___________________
3.__________________________________________ ___________________
4.__________________________________________ ___________________
5.__________________________________________ ___________________
Treating Provider’s Signature: _______________________________________Date: ___________
Completed form can be faxed to:
mailed to: Horizon BCBSNJ, Horizon Behavioral Health PO Box # 4274 Cherry Hill, NJ 08034
Page 1 of 2 The Horizon Behavioral Health program is administered by ValueOptions of New Jersey, Inc.
ABA CONCURRENT SERVICES REQUEST
Please indicate type(s) of service provided by care team in next 6 months and re- quested hours per day and days per week
Program Setting: Home Facility/Clinic School Other:
______________________________________________________________________________________________________________________________________
Adaptive Behavior Treatment (Direct 1:1 ABA Therapy)
∙0364T, 0365T: by technician, receiving 1 hr of supervision for every 5 to 10 hrs of direct treatment.
___ hours per day (based on 30 min. increments), ___ days per week
∙ 0368T, 0369T: by MD/Qualified Health Care Professional (QHCP)
___ hours per day (based on 30 min. increments), ___ days per week
∙0373T, 0374T: Exposure Adaptive Behavior Treatment requiring 2 or more technicians, for severe maladaptive behaviors
___ hours per day (based on an initial 60 minutes with additional 30 minute incre-
ments) by technician, ___ days per week
Group Adaptive Behavior Treatment
∙0372T: Social Skills Group by MD/QHCP,
___ hours per day (based on 30 minute increments), ___ days per week
∙0366T, 0367T: Group Adaptive Behavior Treatment by Protocol by technician,
___ hours per day (based on 30 min. increments), ___ days per week
Assessment /
∙0359T: Behavior Identification Assessment (initial), 60 minute increment
∙0360T/0361T: Observational Behavior
∙0362T/0363T Exposure Behavior
Requested total hours for combined 0359T, 0360T/0361T, 0362T/0362T
Family adaptive behavior treatment guidance by MD/ QHCP, without patient
∙0370T: with individual family.
___ hours per day (based on 30 minute increments), ___ days per week
∙0371T: with multiple family group,
___ hours per day (based on 30 minute increments), ___ days per week
Other _____________________________ frequency:_________________
Patient Name:_______________________________ ID#_____________________
(name and ID are needed to ensure that both pages are for same individual)
Concurrent TREATMENT REPORT
ABA Provider Report Guidelines are available on ValueOptions.com (ATTACH your treatment report ensuring that all required details are covered)
I.
Current Problem Areas/Skill Deficits
∙Social Interaction Impairments
∙Communications Impairments
∙Restricted, repetitive, stereotyped patterns of behavior, interests, and activities
Description of goals achieved within the recent authorization period
Summary of Family/Caregiver Involvement and Plan for Continued Participation/ Behavioral Management Skill Transfer
II.TREATMENT
Treatment Description
∙Instructional Methods (ie DTT, PRT, Natural Environment
∙Behavioral Methods (DRA, DRO, Behavioral Momentum
∙Treatment Setting
∙Description of supervision and direct service delivery process (who/what/when and
∙frequency)
∙Description of care coordination activities
∙Summary of services delivered to
New or continued measurable objectives to address both behavior & skill deficits:
∙Conditions in which skill/behavior is to occur, including generalized settings
∙Behavioral definition of desired skill(s)/behavior(s) - observable and measurable
∙Baseline data (attach graphic display)
∙Current results data (attach graphic display)
∙Behavior mastery criteria (quantify frequency and settings to demonstrate mastery)
∙Recommendation/justification for continued treatment
∙Skill(s) introduction target date
∙Skill(s) mastery target date
Page 2 of 2 The Horizon Behavioral Health program is administered by ValueOptions of New Jersey, Inc. revised 11/24/2014