

Fill out the AIMS assessment PDF online using our PDFinity® editor. The editor works on any device and lets you complete, save, and download the form in minutes. Follow these steps to get started:
Step 1: First, access the editor by pressing the "Get Form Button" at the top of this page.
Step 2: This editor offers the capability to customize almost all PDF forms in a range of ways. Transform it by writing any text, correct existing content, and place in a signature - all manageable within a few minutes!
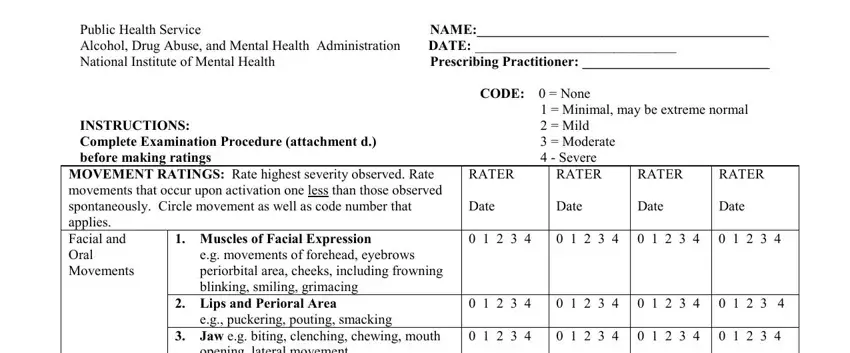
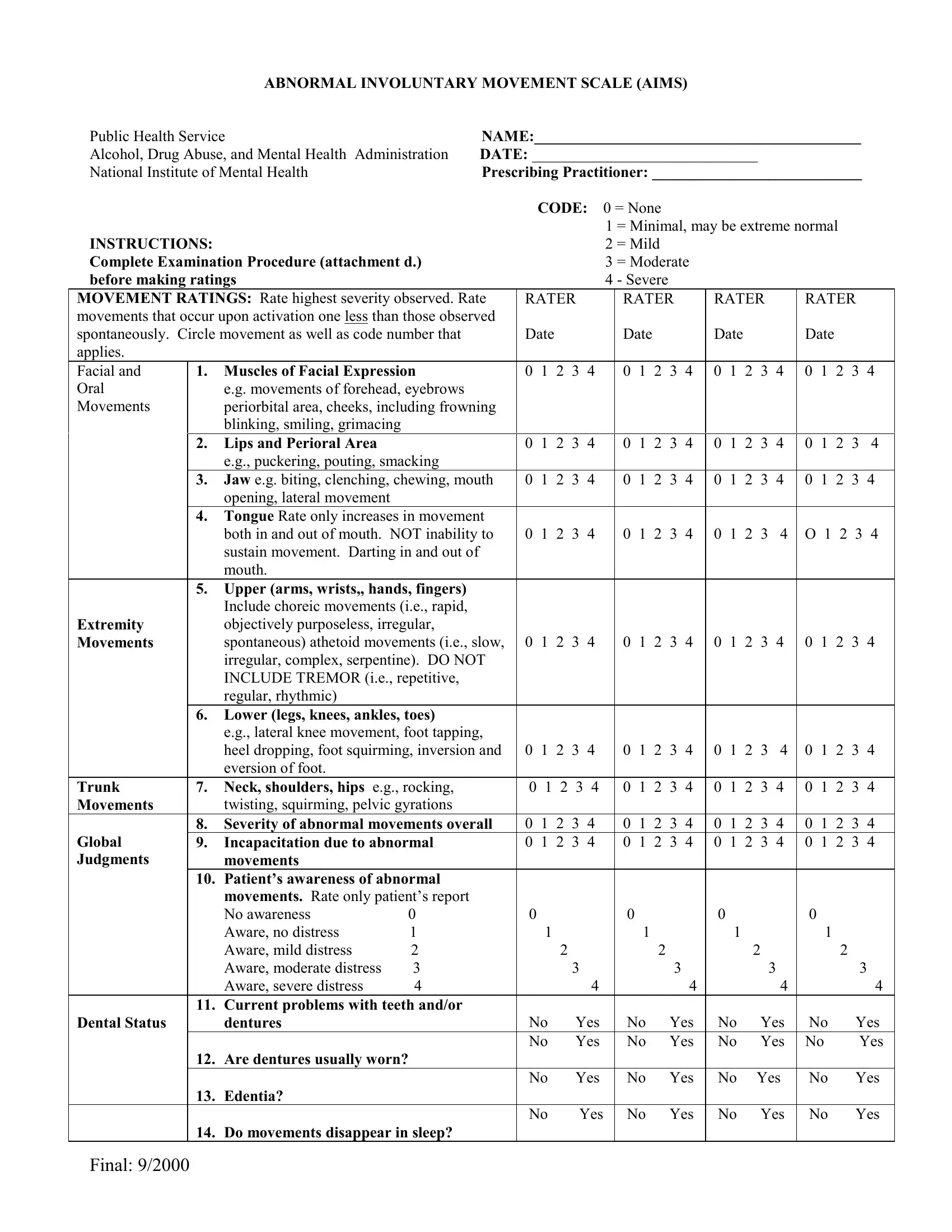
2. After completing the first section, insert the required details in the extremity movement fields: lateral movement, tongue rate, upper arm and wrist movements, lower leg and knee movements, and trunk movements including neck, shoulder, and hip areas. Also complete the Global Judgments section covering the severity of abnormal movements and the patient's awareness of those movements.
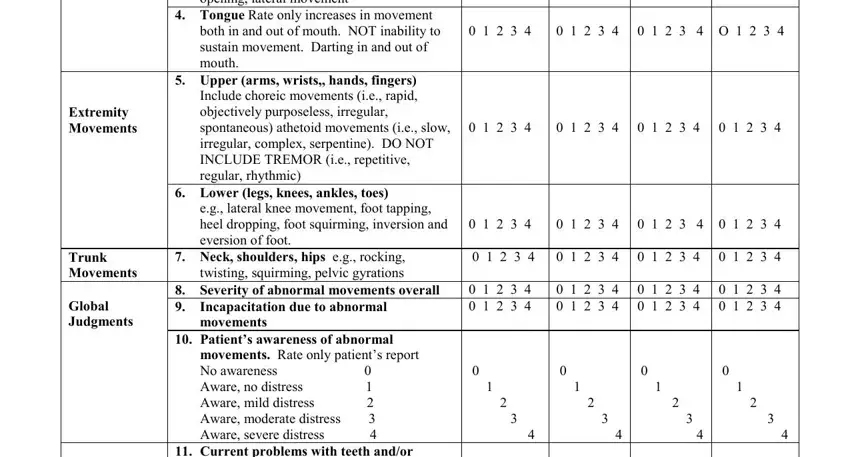
Take care to review the severity of abnormal movements section before finalizing, as errors here are the most common mistake when completing the AIMS form.
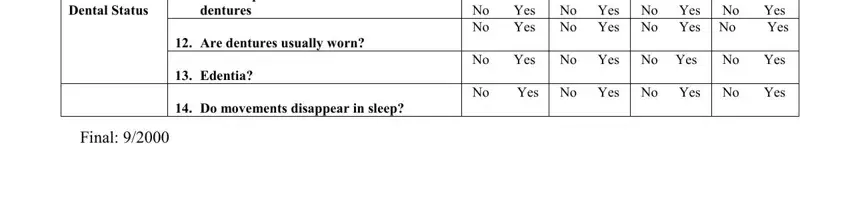
3. In this final step, fill out the dental status fields: current problems with teeth or dentures, whether dentures are usually worn, edentulous status, and whether movements disappear during sleep. Mark each Yes or No response carefully.
Step 3: Before submitting the file, confirm that all form fields have been completed correctly. Once everything looks right, click "Done." With a 7-day free trial account, you can download the aims assessment PDF or email it right away. FormsPal uses a secure system that never records or shares your sensitive information. Need a related tool? Explore the Functional Independence Measure (FIM) Scale for functional capacity assessment.