
 Continue sending my check to the bank.
Continue sending my check to the bank.Completing the NYCERS Change of Address Form online is fast and simple. The free PDF editor lets you fill in all required fields, save your form, and print a copy ready for notarization.
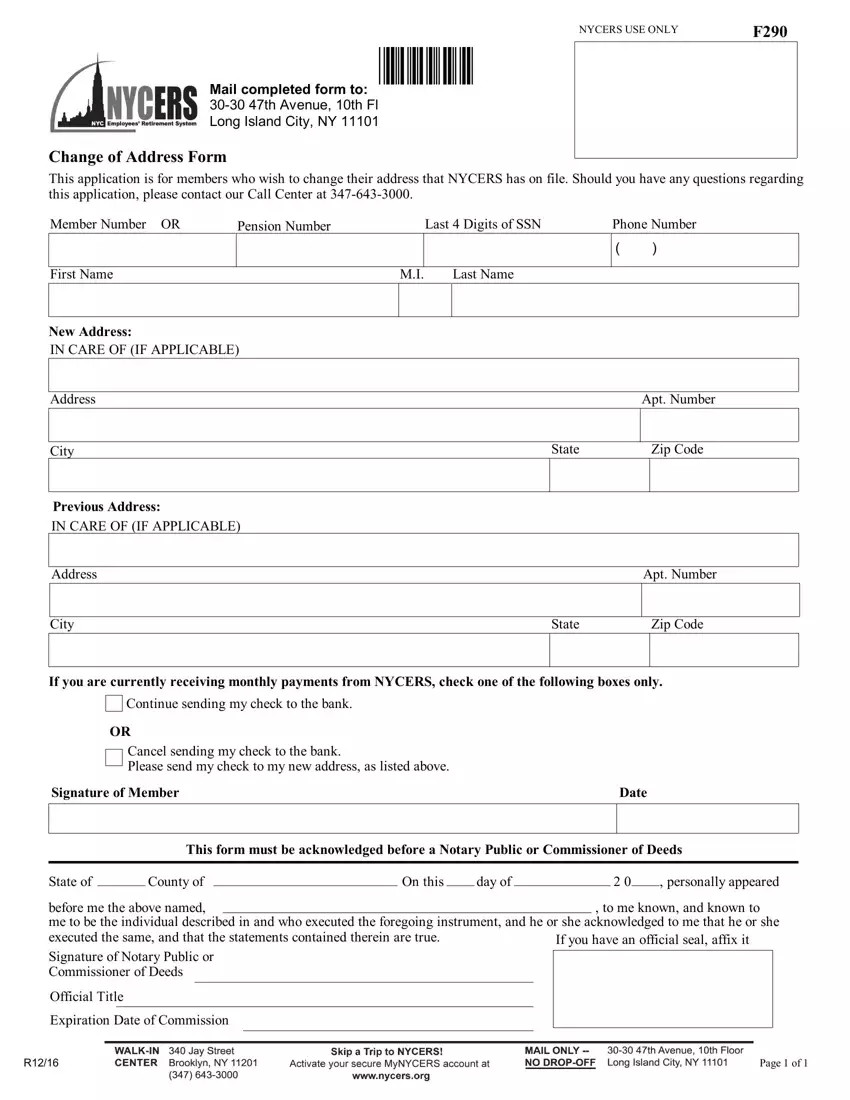
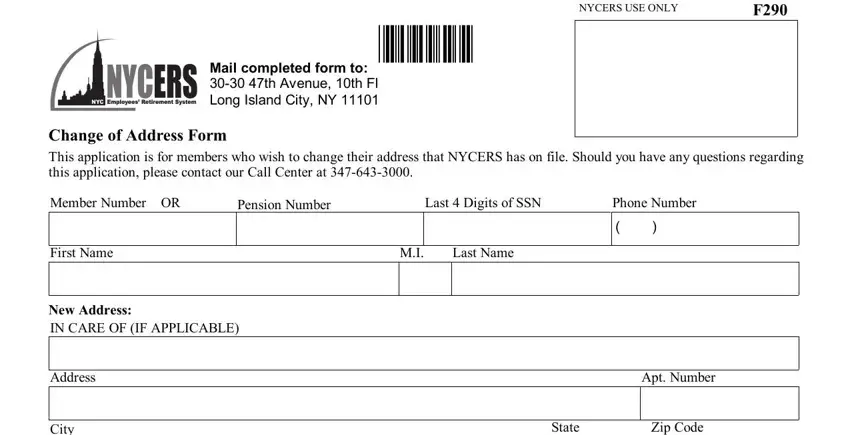
Step 1: Open the Form. Click the "Get Form Here" button at the top of the page to launch the online PDF editor. No registration or software download is required.
Step 2: Enter Your Personal and Address Information. On the editing page, click each field to enter your details. You can type directly into any field, add check marks, highlight text, and insert your signature. The fields in the upper section of the form include your name, NYCERS member number, and both your old and new mailing addresses, including apartment number, city, state, and ZIP code.
Step 3: Complete the Payment Routing Section. If you receive monthly pension payments by check, use the checkboxes in the middle section to indicate whether to continue sending your check to the new address or cancel check delivery. Enter your signature and the date on the member signature line. This section also includes fields for the city, state, and ZIP code associated with your payment address.
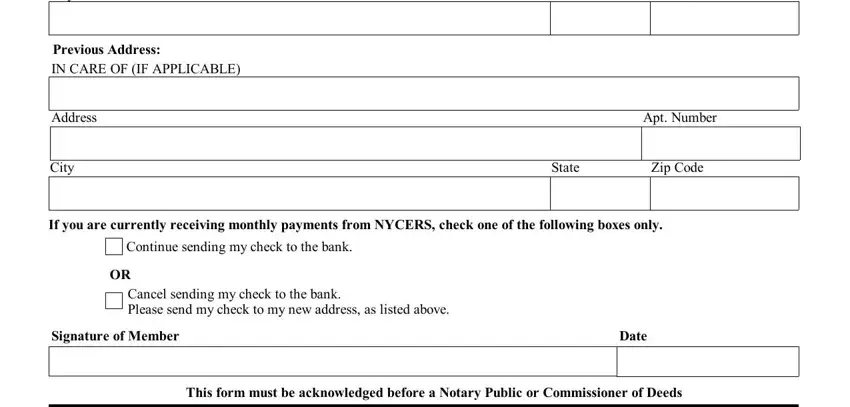
Step 4: Get the Form Notarized. Print your completed form and take it to a Notary Public or Commissioner of Deeds. The notary fills in the bottom section with the state, county, and date, along with their official title, seal, and commission expiration date. Most NYC banks and public libraries offer free notary services.
Step 5: Save and Submit. Click "Done" to download your completed form. Print at least two copies, one to submit and one for your records. Mail or hand-deliver your original notarized form to NYCERS. NYCERS does not accept submissions by fax or email.
Looking for related address and retirement forms?
