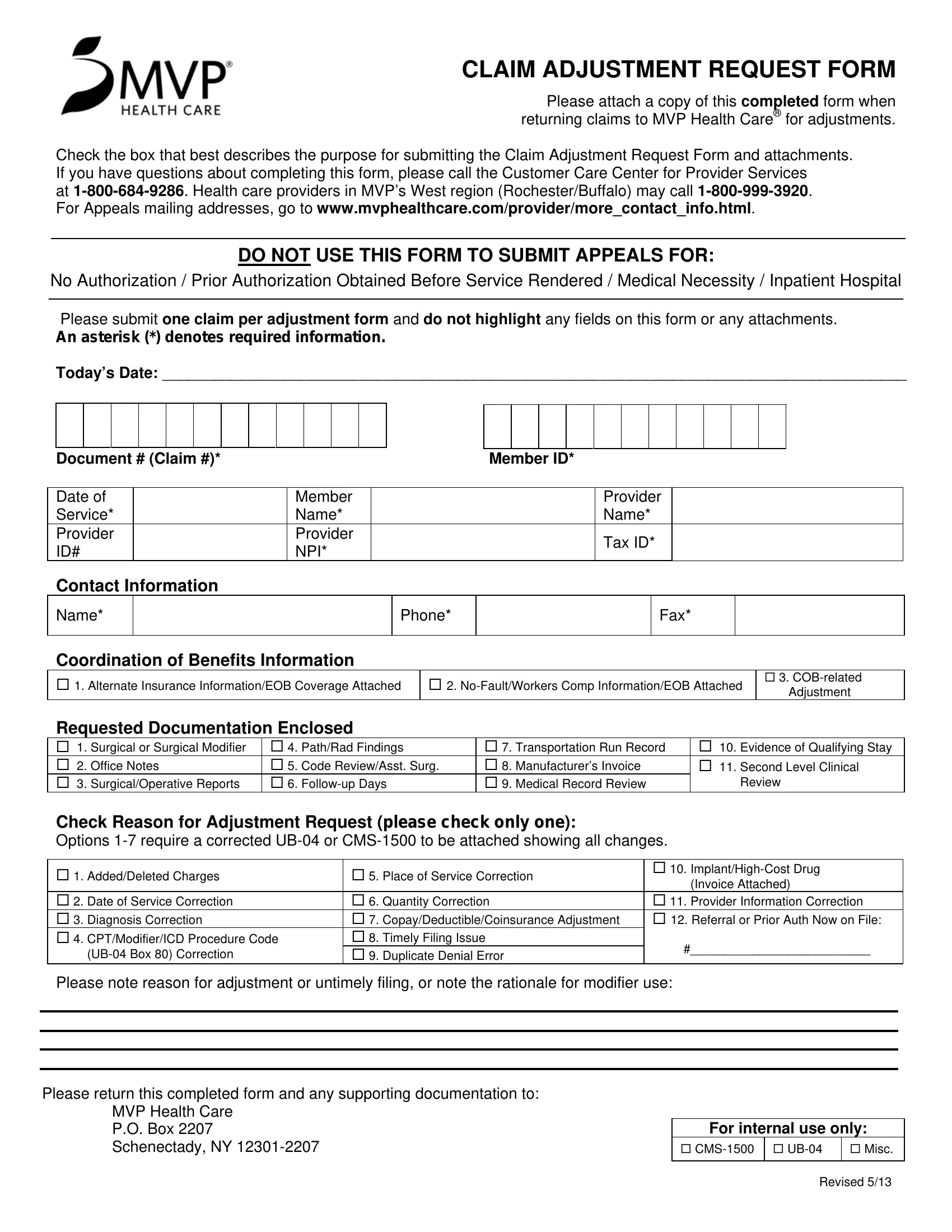

Follow these steps to complete your adjustment request for MVP Health Care.
- Identify the reason. Select the correct reason code on the form, such as date of service correction, procedure code change, diagnosis correction, or coordination of benefits.
- Complete required fields. Fill in all fields marked with an asterisk, including the provider NPI, patient name, claim number, and service date.
- Attach supporting documents. Include a corrected UB-04 or CMS-1500 for billing corrections, or the other carrier's explanation of benefits for coordination of benefits issues.
- Submit one claim per form. Each adjustment must be on a separate form. Do not combine multiple claims on one submission.
- Mail to MVP Health Care. Send the completed form and attachments to the appropriate address shown on the form.
View related forms: CMS-1450 Claim Form, Medical Claim Form, and Aetna Appeal Form.