

You can complete this adult emergency form online using our PDFinity® editor. Follow these steps to fill it out accurately and completely.
Steps to Fill Out the Adult Emergency Form
Step 1: Click the "Get Form" button at the top of this page to open the editor.
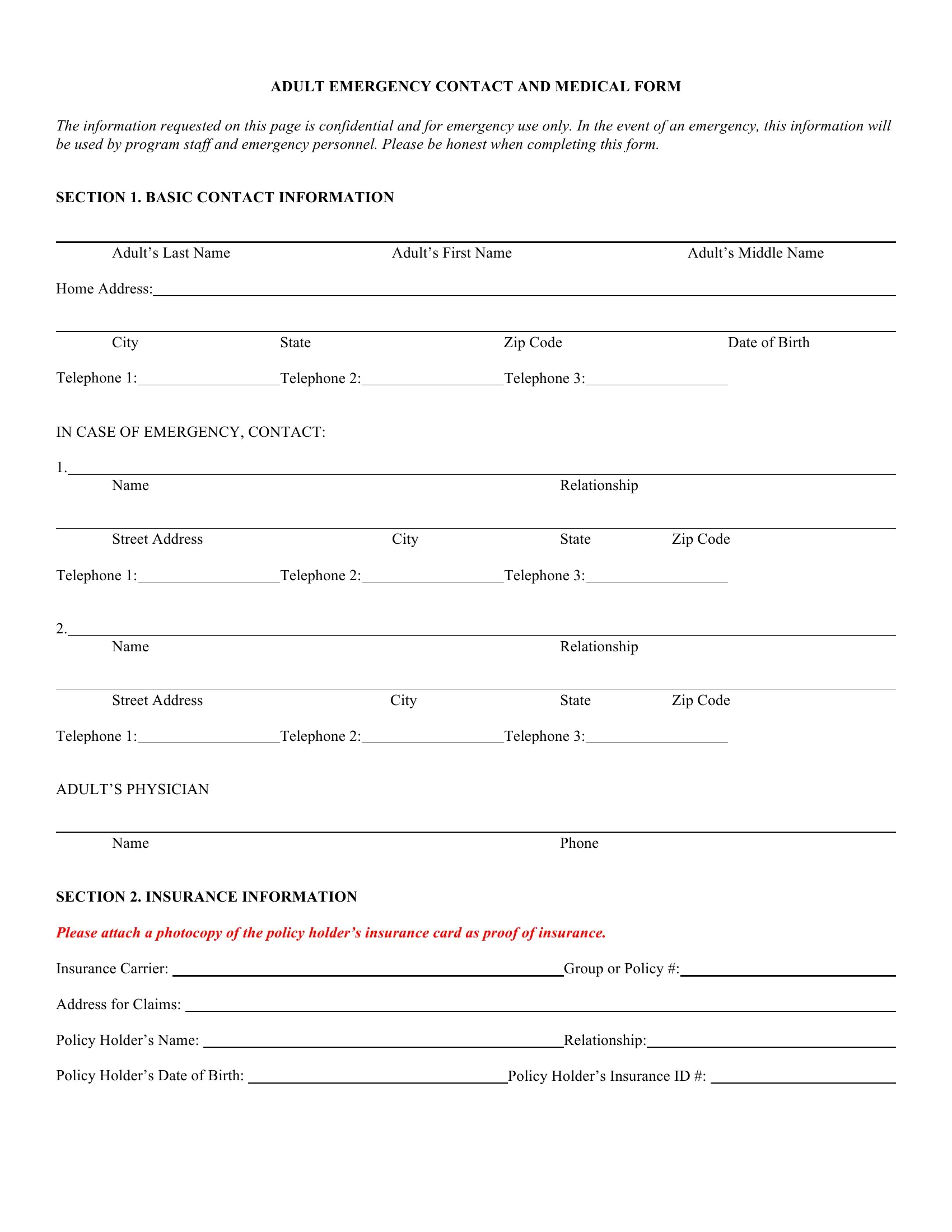
Step 2: Add your personal details in the first section, including your full name, home address, date of birth, and contact phone numbers. Fill every field - incomplete contact information makes the form less useful in an emergency.
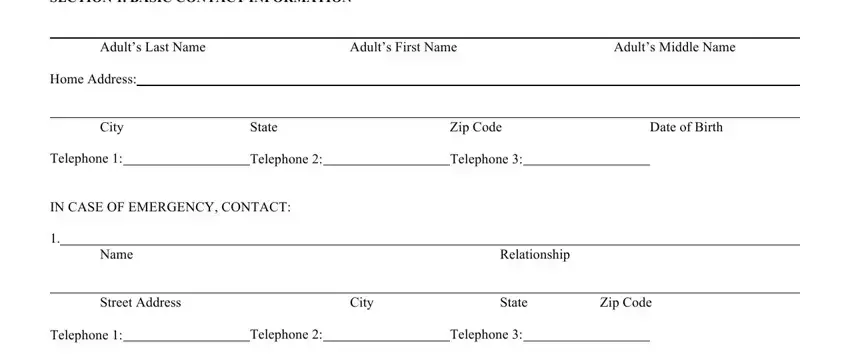
Step 3: Enter your emergency contacts. Include their name, relationship to you, and at least two reliable phone numbers so coordinators can always reach someone.
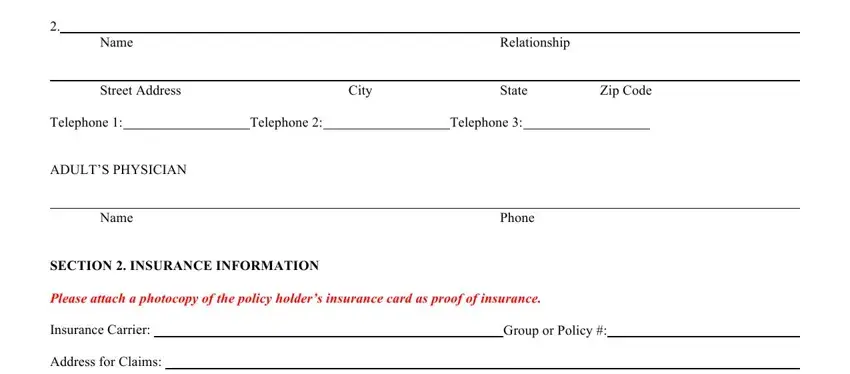
Step 4: Complete the insurance information section with your policy holder name, carrier name, group number, and insurance ID. Attaching a copy of your insurance card is recommended where possible.
Step 5: Fill in the health information section. List all allergies, current medications with dosages, and any pre-existing conditions. These fields are required - accurate health information allows first responders to deliver faster and safer care.
Step 6: Review the treatment authorization clause and any liability or photo release language, then print your name, sign, and date the form.

Step 7: Click "Done," then download or print your completed form. Sign up for a free FormsPal account to save the file and return to update it whenever your health information changes.
Frequently Asked Questions
Who needs an adult emergency form?
Adults joining organized programs, camps, sports leagues, or care facilities typically must complete an emergency form before participating. Coordinators use it to reach designated contacts and inform medical staff of health conditions during a crisis.
What should I include in the medical history section?
List all known allergies (food, medications, and environmental), all current prescription and over-the-counter medications with dosages, and any chronic conditions such as asthma, diabetes, or heart disease. Leaving these fields blank can delay or complicate emergency treatment.
How often should I update my adult emergency form?
Review and update your form whenever your health information changes - for example, after starting a new medication or receiving a new diagnosis. Keeping emergency contact numbers current is equally important. You can return to FormsPal at any time to edit your saved copy.
What other safety documents should I keep on file?
An adult emergency form works best alongside a portable emergency card. For longer-term health planning, consider also filing a Living Will or Medical Power of Attorney to document your medical preferences in advance.