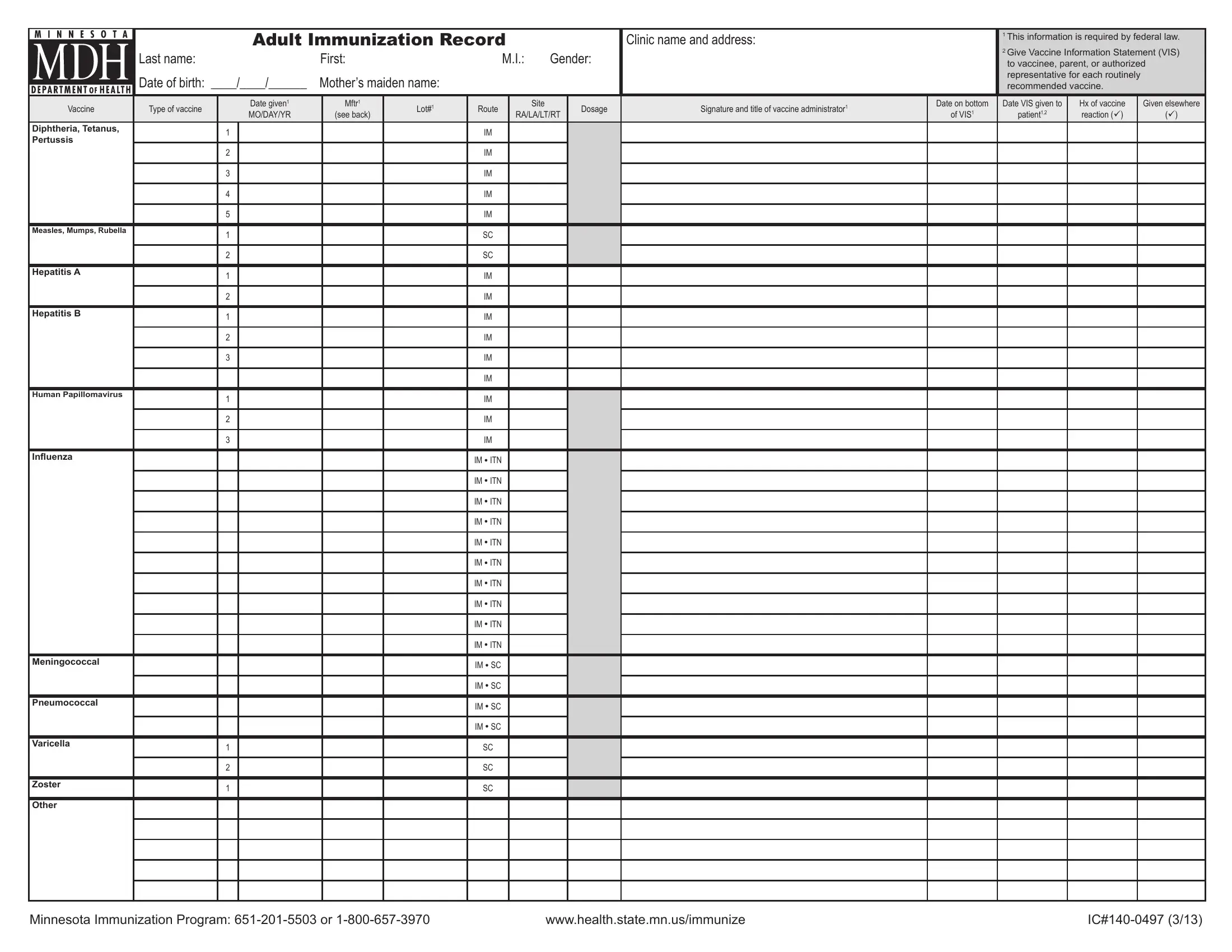
An Adult Immunization Record is an essential tool designed to keep track of vaccinations for adults, ensuring they are up-to-date with their immunizations. This detailed form captures a wide array of information, beginning with basic personal details like last name, first name, middle initial, gender, date of birth, and mother’s maiden name. For healthcare providers, it's a pivotal document that includes the clinic's name and address, emphasizing the importance of accessible patient vaccination records. By federal law, specific information such as the vaccine type, the manufacturer, lot number, route and site of administration, dosage, the administrator's signature and title, and dates regarding when the vaccine was given and the Vaccine Information Statement (VIS) was provided, must be meticulously logged. This record not only facilitates the provision of information required under the National Childhood Vaccine Injury Act for adult vaccinations but also aids in monitoring adherence to recommended immunization schedules. It outlines the appropriate method to record combination vaccines, injection routes, and sites, which is crucial for effective vaccine delivery and minimizing adverse reactions. Furthermore, the form provides guidance on how to document vaccine reactions and transferring immunization information, ensuring a comprehensive vaccination history that can be shared across healthcare providers. It also introduces the Minnesota Immunization Information Connection (MIIC) and underscores the importance of manufacturer codes for accurate vaccine identification. Ultimately, the Adult Immunization Record serves as a vital document for managing and promoting the health and wellness of individuals through vaccination.
| Question | Answer |
|---|---|
| Form Name | Adult Immunization Record Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | MIIC, minnesota adult immunization record, adult immunization record, immunization records for adults |
ADULT IMMUNIZATION RECORD
Last name: |
First: |
M.I.: |
Gender: |
Date of birth: ____/____/______ |
Mother’s maiden name: |
|
|
Clinic name and address:
1This information is required by federal law.
2Give Vaccine Information Statement (VIS) to vaccinee, parent, or authorized representative for each routinely recommended vaccine.
Vaccine |
Type of vaccine |
|
Date given1 |
Mftr1 |
Lot#1 |
Route |
Site |
Dosage |
Signature and title of vaccine administrator1 |
Date on bottom |
Date VIS given to |
Hx of vaccine |
Given elsewhere |
|
MO/DAY/YR |
(see back) |
RA/LA/LT/RT |
of VIS1 |
patient1,2 |
reaction (ü) |
(ü) |
||||||
|
|
|
|
|
|
|
|||||||
Diphtheria, Tetanus, |
|
1 |
|
|
|
IM |
|
|
|
|
|
|
|
Pertussis |
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
|
|
|
IM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
|
|
|
IM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4 |
|
|
|
IM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5 |
|
|
|
IM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Measles, Mumps, Rubella |
|
1 |
|
|
|
SC |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
|
|
|
SC |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hepatitis A |
|
1 |
|
|
|
IM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
|
|
|
IM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hepatitis B |
|
1 |
|
|
|
IM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
|
|
|
IM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
|
|
|
IM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
IM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Human Papillomavirus |
|
1 |
|
|
|
IM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
|
|
|
IM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
|
|
|
IM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Inluenza |
|
|
|
|
|
IM ● ITN |
|
|
|
|
|
|
|
|
|
|
|
|
|
IM ● ITN |
|
|
|
|
|
|
|
|
|
|
|
|
|
IM ● ITN |
|
|
|
|
|
|
|
|
|
|
|
|
|
IM ● ITN |
|
|
|
|
|
|
|
|
|
|
|
|
|
IM ● ITN |
|
|
|
|
|
|
|
|
|
|
|
|
|
IM ● ITN |
|
|
|
|
|
|
|
|
|
|
|
|
|
IM ● ITN |
|
|
|
|
|
|
|
|
|
|
|
|
|
IM ● ITN |
|
|
|
|
|
|
|
|
|
|
|
|
|
IM ● ITN |
|
|
|
|
|
|
|
|
|
|
|
|
|
IM ● ITN |
|
|
|
|
|
|
|
Meningococcal |
|
|
|
|
|
IM ● SC |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
IM ● SC |
|
|
|
|
|
|
|
Pneumococcal |
|
|
|
|
|
IM ● SC |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
IM ● SC |
|
|
|
|
|
|
|
Varicella |
|
1 |
|
|
|
SC |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
|
|
|
SC |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Zoster |
|
1 |
|
|
|
SC |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Minnesota Immunization Program: |
www.health.state.mn.us/immunize |

How to use MDH’s Adult Immunization Record form
Make this record easily accessible
Keep each patient’s immunization record where you can easily review it during each ofice visit (e.g., the front inside cover of the patient’s medical
chart).
Patient behind schedule?
Flag the record if the patient is behind on recommended immunizations.
Record type of vaccine
Be sure to indicate the type of vaccine you gave. This is especially important when you give Tdap rather than Td since persons who receive Td will be at higher risk of pertussis disease if there is a pertussis outbreak in the community.
What information is required by federal law?
You are required by federal law to record the following information as part of the National Childhood Vaccine Injury Act, even though you are administering vaccines to adult patients:
•Manufacturer and lot number of vaccine given.
•Date vaccine given.
•Date of publication of the Vaccine Information Statement (VIS) and the date the VIS was given to the vaccinee.
•Name, title, and address of the person who administered the vaccine.
Note: Federal and Minnesota laws do not require written informed consent. However, some clinics may have their own policy.
How to record combination vaccines
Record a combination vaccine under each speciic antigen that the vaccine contains. Use a hyphen between each antigen. For example:
•Twinrix is
How to record injection routes and sites
The most common routes for vaccination are intramuscular (IM) and subcutaneous (SC or SQ). Less frequent routes include oral (PO) and intranasal (ITN). If there is more than one choice for route, circle the route given. Sites for injections should be noted as to which limb and what side. These include right arm (RA) and left arm (LA), and when necessary, right thigh (RT) and left thigh (LT).
Immunization Program P.O. Box 64975
St. Paul, MN
Hx of vaccine reaction (history of vaccine reaction)
If the patient has experienced a clinically signiicant or unexpected event after an immunization (even if there is uncertainty that the vaccine caused
the event), place a ü in the “Hx of vaccine reaction” column. Provide more speciics about that event elsewhere in the patient’s chart. Report vaccine
reactions to the Vaccine Adverse Events Reporting System (http://vaers.hhs.gov or
Transferring immunization information onto this form
Transfer vaccine information that patients receive at other clinics to this record. If you don’t know all of the information, record at least the date (mo/ day/yr) and type of vaccine. The responsibility for maintaining the federally required information is with the clinic that administered the vaccine. Be sure to place a ü in the “Given elsewhere” column. If a patient transfers to another clinic, provide a photocopy to the new clinic.
Use the MIIC registry to record and ind immunizations
If you’re participating in the Minnesota Immunization Information Connection (MIIC), be sure to enter or submit data on new shots for this patient so it is available to others who may be giving subsequent doses. MIIC is located at https://miic.health.state.mn.us. If you are not yet participating, call
Registry”) to ind out how to enroll.
Manufacturers’ codes
Use the codes listed in the chart below to indicate the manufacturer of the vaccine. These are the same codes used universally and by the Minnesota Immunization Information Connection (MIIC).
Vaccine Manufacturer |
Code |
CSL Biotherapies |
CSL |
|
|
GlaxoSmithKline |
SKB |
|
|
Massachusetts Biologic Labs |
MBL |
|
|
MedImmune, Inc. |
MED |
|
|
Merck & Co., Inc. |
MSD |
|
|
Novartis |
NOV |
|
|
sanoi pasteur Inc. |
PMC |
Pizer Vaccines |
WAL |
Your patients need personal immunization record cards
Always update the patient’s personal immunization record with information on the vaccines that you administered. If your clinic needs personal immunization record cards, order the MDH Gold Card by calling
5503, or by illing out the order form at www.health.state.mn.us/immunize.