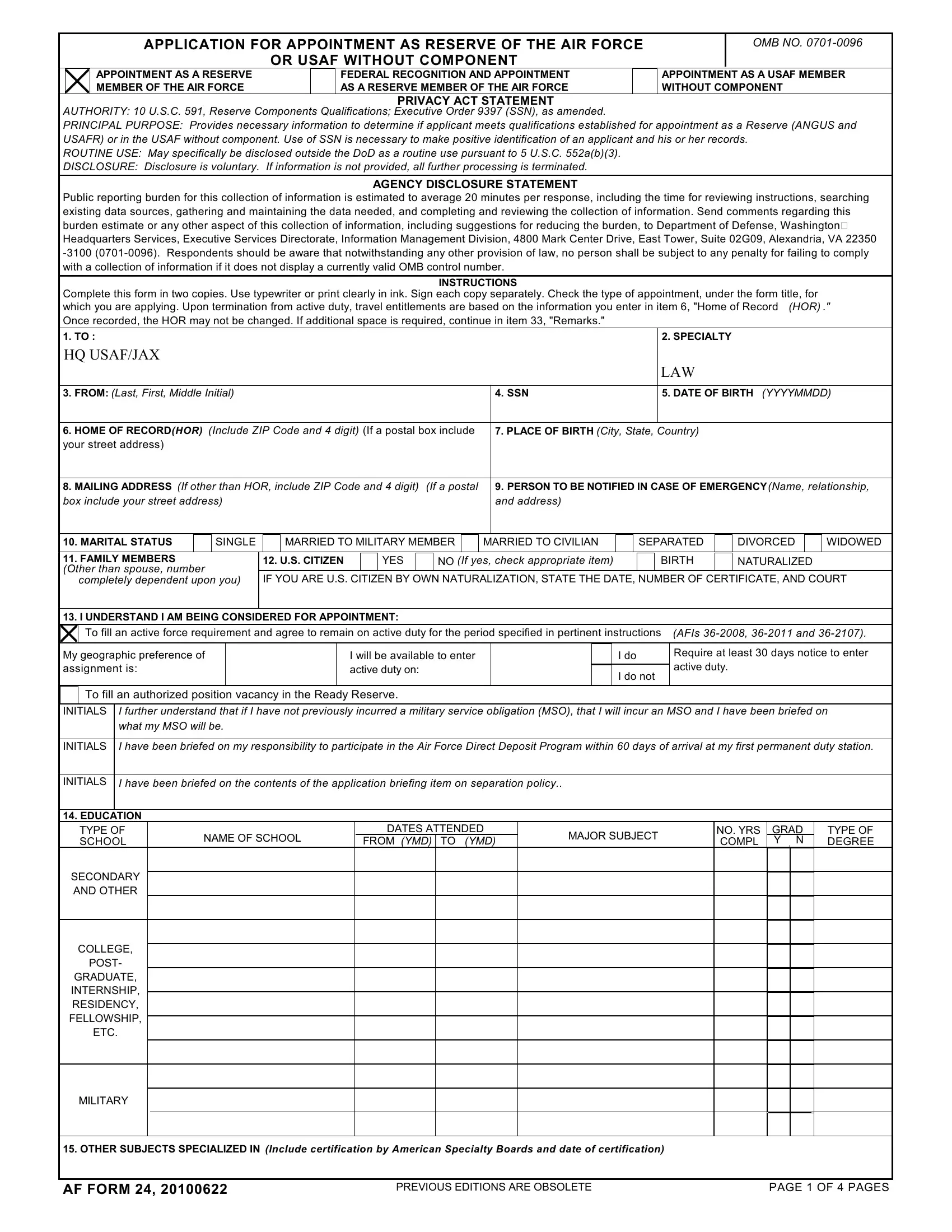
The AF 24 form serves as a critical document for individuals seeking appointment as a Reserve of the Air Force or as a USAF member without component. This form is instrumental in the evaluation process, providing a comprehensive overview of the applicant's background, qualifications, and suitability for serving in the military capacity they aspire to. By collecting detailed information ranging from personal identification, educational background, to previous service and medical history, the AF 24 form ensures that only those who meet the established qualifications are considered for appointment. The form also includes sections that address legal and ethical considerations, such as past convictions or disciplinary actions, which are imperative for maintaining the integrity and standards of the Air Force. Additionally, it touches on the applicant’s willingness and readiness to partake in the Air Force Direct Deposit Program, a reflection of the detailed and thorough nature of the application process designed to vet candidates comprehensively. Privacy and disclosure statements included in the document highlight the importance of confidentiality and voluntary disclosure, respecting applicants' privacy while also ensuring that the selection process is informed and fair. With an estimated average completion time, the AF 24 form underscores the Department of Defense's commitment to efficiency and consideration for applicants' time, further exemplified by the encouragement of comments or suggestions aimed at reducing the burden on applicants. This structured and detailed approach facilitates a transparent, efficient, and fair selection process, essential for upholding the high standards expected of Air Force personnel.
| Question | Answer |
|---|---|
| Form Name | Af Form 24 |
| Form Length | 5 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min 15 sec |
| Other names | form 24 pdf, form 24 download, af form 24 fillable, af form 24 |
APPLICATION FOR APPOINTMENT AS RESERVE OF THE AIR FORCE
OR USAF WITHOUT COMPONENT
OMB NO.
APPOINTMENT AS A RESERVE MEMBER OF THE AIR FORCE
FEDERAL RECOGNITION AND APPOINTMENT AS A RESERVE MEMBER OF THE AIR FORCE
APPOINTMENT AS A USAF MEMBER WITHOUT COMPONENT
PRIVACY ACT STATEMENT
AUTHORITY: 10 U.S.C. 591, Reserve Components Qualifications; Executive Order 9397 (SSN), as amended.
PRINCIPAL PURPOSE: Provides necessary information to determine if applicant meets qualifications established for appointment as a Reserve (ANGUS and USAFR) or in the USAF without component. Use of SSN is necessary to make positive identification of an applicant and his or her records.
ROUTINE USE: May specifically be disclosed outside the DoD as a routine use pursuant to 5 U.S.C. 552a(b)(3).
DISCLOSURE: Disclosure is voluntary. If information is not provided, all further processing is terminated.
AGENCY DISCLOSURE STATEMENT
Public reporting burden for this collection of information is estimated to average 20 minutes per response, including the time for reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information. Send comments regarding this burden estimate or any other aspect of this collection of information, including suggestions for reducing the burden, to Department of Defense, Washington Headquarters Services, Executive Services Directorate, Information Management Division, 4800 Mark Center Drive, East Tower, Suite 02G09, Alexandria, VA 22350
INSTRUCTIONS
Complete this form in two copies. Use typewriter or print clearly in ink. Sign each copy separately. Check the type of appointment, under the form title, for which you are applying. Upon termination from active duty, travel entitlements are based on the information you enter in item 6, "Home of Record (HOR) ." Once recorded, the HOR may not be changed. If additional space is required, continue in item 33, "Remarks."
1. TO : |
2. SPECIALTY |
HQ USAF/JAX |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LAW |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3. FROM: (Last, First, Middle Initial) |
|
|
|
|
|
|
|
|
|
|
4. SSN |
|
|
|
5. DATE OF BIRTH (YYYYMMDD) |
||||||
6 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6. HOME OF RECORD(HOR) (Include ZIP Code and 4 digit) (If a postal box include |
|
7. PLACE OF BIRTH (City, State, Country) |
|
|
|
|
|||||||||||||||
your street address) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
8 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
8. MAILING ADDRESS (If other than HOR, include ZIP Code and 4 digit) |
(If a postal |
|
9. PERSON TO BE NOTIFIED IN CASE OF EMERGENCY(Name, relationship, |
||||||||||||||||||
box include your street address) |
|
|
|
|
|
|
|
|
|
|
and address) |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10. MARITAL STATUS |
|
SINGLE |
|
|
MARRIED TO MILITARY MEMBER |
|
MARRIED TO CIVILIAN |
|
|
SEPARATED |
|
DIVORCED |
|
WIDOWED |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
11. FAMILY MEMBERS |
|
|
12. U.S. CITIZEN |
|
YES |
|
|
NO (If yes, check appropriate item) |
|
|
|
BIRTH |
|
NATURALIZED |
|
||||||
(Other than spouse, number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
IF YOU ARE U.S. CITIZEN BY OWN NATURALIZATION, STATE THE DATE, NUMBER OF CERTIFICATE, AND COURT |
|||||||||||||||||||
completely dependent upon you) |
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
13. I UNDERSTAND I AM BEING CONSIDERED FOR APPOINTMENT:
|
|
To fill an active force requirement and agree to remain on active duty for the period specified in pertinent instructions |
(AFIs |
||||
|
|
|
|
|
|
|
|
|
My geographic preference of |
I will be available to enter |
|
I do |
Require at least 30 days notice to enter |
||
|
assignment is: |
|
|
|
|
active duty. |
|
|
active duty on: |
|
I do not |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
To fill an authorized position vacancy in the Ready Reserve.
INITIALS |
I further understand that if I have not previously incurred a military service obligation (MSO), that I will incur an MSO and I have been briefed on |
|
what my MSO will be. |
|
|
INITIALS |
I have been briefed on my responsibility to participate in the Air Force Direct Deposit Program within 60 days of arrival at my first permanent duty station. |
INITIALS
I have been briefed on the contents of the application briefing item on separation policy..
14. EDUCATION
TYPE OF |
NAME OF SCHOOL |
DATES ATTENDED |
MAJOR SUBJECT |
NO. YRS |
GRAD |
TYPE OF |
|
SCHOOL |
FROM (YMD) TO (YMD) |
COMPL |
Y N |
DEGREE |
|||
|
|||||||
SECONDARY |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
AND OTHER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
COLLEGE, |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
POST- |
|
|
|
|
|
|
|
GRADUATE, |
|
|
|
|
|
|
|
INTERNSHIP, |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
RESIDENCY, |
|
|
|
|
|
|
|
FELLOWSHIP, |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
ETC. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MILITARY
15. OTHER SUBJECTS SPECIALIZED IN (Include certification by American Specialty Boards and date of certification)
AF FORM 24, 20100622
PREVIOUS EDITIONS ARE OBSOLETE |
PAGE 1 OF 4 PAGES |
16. PHYSICIANS ONLY |
|
I DO |
DO NOT DESIRE TRAINING IN AVIATION MEDICINE |
17. CHRONOLOGICAL STATEMENT OF SERVICE AND TRAINING IN ANY COMPONENT OF THE UNIFORMED SERVICES(Include service academies and
preparatory schools, Reserve Officer Training Crops (ROTC), Officer Training School (OTS), Health Professions Scholarship (HPSP), etc.)
|
DATES ATTENDED |
|
|
HIGHEST |
|
ORGANIZATION |
|
|
|
SPECIALTY |
|
ACTIVE DUTY |
|||||
FROM (YMD) |
TO (YMD) |
GRADE |
|
(Type and Service) |
|
|
|
|
OR RESERVE |
||||||||
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
18. ARE YOU CURRENTLY A MEMBER OF ANY BRANCH OF THE UNIFORMED SERVICES? |
19. WERE ALL DISCHARGES HONORABLE? |
||||||||||||||||
|
|
YES |
|
|
NO |
(If yes, provide branch of uniformed service) |
|
|
|
|
YES |
|
NO |
||||
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
20. WERE YOU EVER NONSELECTED FOR PROMOTION TO AN OFFICER GRADE IN ANY BRANCH OF THE UNIFORMED SERVICES? |
|
|
|||||||||||||||
|
|
YES |
|
|
NO |
(If yes, provide branch of uniformed service) |
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
21. WERE YOU SEPARATED OR ARE YOU PENDING SEPARATION FROM ANY BRANCH OF THE UNIFORMED SERVICES FOR CAUSE, OR WERE YOU SEPARATED OR ARE YOU PENDING SEPARATION FROM COMMISSIONED STATUS IN ANY BRANCH OF THE UNIFORMED SERVICES DUE TO NONQUALIFIED, NONSELECT, OR DEFERRAL PROMOTION?
YES |
|
NO (If yes, provide branch of uniformed service, reason for separation action, and date of separation, if applicable) |
22. HAVE YOU EVER RECEIVED SEVERANCE PAY, OR SEPARATION PAY, OR READJUSTMENT PAY, OR VOLUNTARY SEPARATION INCENTIVE(VSI) OR SPECIAL SEPARATION BENEFIT(SSB) PAY WHEN RELEASED FROM ACTIVE DUTY OR DISCHARGED FROM ANY UNIFORMED SERVICE?
|
|
YES |
|
NO |
||||
|
|
|
|
|
||||
|
|
|
||||||
23. HAVE YOU PREVIOUSLY MADE APPLICATION AND BEEN REJECTED FOR COMMISSIONING BY ANY COMPONENT OF THE UNIFORMED SERVICES? |
||||||||
|
|
YES |
|
NO (If yes, please state when and where rejected, and cause) |
||||
|
|
|
||||||
|
|
|
|
|
||||
|
||||||||
24. HAVE YOU EVER APPLIED FOR A COMMISSION OR POSITION WITH ANY BRANCH OF THE ARMED SERVICES OR FEDERAL GOVERNMENT? IF SO, PLEASE |
||||||||
EXPLAIN. |
|
YES |
|
|
NO (If additional space is required, continue in "REMARKS") |
|||
|
|
|
||||||
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
25. CHRONOLOGICAL STATEMENT OF CIVILIAN EMPLOYMENT, INCLUDING
|
FROM (YMD) |
TO (YMD) |
|
EMPLOYED BY (Give name and address to include ZIP Code and 4 digit) |
FULL |
PART TIME |
MONTHLY SALARY |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
TIME |
(Hrs per week) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
POSITION AND DUTIES |
|
|
|
|
|
REASON FOR TERMINATION |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FROM (YMD) |
TO (YMD) |
|
EMPLOYED BY (Give name and address to include ZIP Code and 4 digit) |
FULL |
PART TIME |
MONTHLY SALARY |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
TIME |
(Hrs per week) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
POSITION AND DUTIES |
|
|
|
|
|
REASON FOR TERMINATION |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FROM (YMD) |
TO (YMD) |
|
EMPLOYED BY (Give name and address to include ZIP Code and 4 digit) |
FULL |
PART TIME |
MONTHLY SALARY |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
TIME |
(Hrs per week) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
POSITION AND DUTIES |
|
|
|
|
|
REASON FOR TERMINATION |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
26. HAVE YOU EVER BEEN INVOLVED, ARRESTED, INDICTED, OR CONVICTED(INCLUDING PRETRIAL DIVERSION) FOR ANY VIOLATION OF CIVIL OR |
|||||||||||||||
|
MILITARY LAW, INCLUDING NONJUDICIAL PUNISHMENT PURSUANT TO ARTICLE 15 OF THE UCMJ, OR MINOR TRAFFIC VIOLATIONS? |
|
|||||||||||||
|
|
YES |
|
|
NO (If yes, please explain below. List all offenses charged against you regardless of final disposition, including situations where the |
||||||||||
|
|
|
|
||||||||||||
|
|
|
|
|
|
involvement has not been recorded locally or the record has been ordered sealed or expunged by the court.) |
|
||||||||
|
|
|
|
|
|
|
|||||||||
|
|
OFFENSE |
|
|
|
DATE |
PLACE |
AGE |
DISPOSITION OF CHARGE |
|
|
COURT |
|||
|
|
|
|
(YYYYMMDD) |
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
AF FORM 24, 20100622 |
PREVIOUS EDITIONS ARE OBSOLETE |
PAGE 2 OF 4 PAGES |
26A. HAVE YOU EVER BEEN CONVICTED OF A DUI OR ALCOHOL RELATED OFFENSE? |
|
|
||||||||
|
|
YES |
|
NO (If yes, submit a statement in your own words describing the circumstances, and a copy of the police report. |
|
|||||
|
|
|
|
|||||||
|
|
|
|
|
involvement has not been recorded locally or the record has been ordered sealed or expunged by the court.) |
|
||||
|
|
OFFENSE |
|
DATE |
PLACE |
AGE |
|
DISPOSITION OF CHARGE |
COURT |
|
|
|
|
(YYYYMMDD) |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
27.ARE YOU A CONSCIENTIOUS OBJECTOR?(A conscientious objector is defined as: One who has or has a firmed, fixed, and sincere objection to participation in war in any form or to bearing of arms because of religious training or belief, which includes solely moral or ethical beliefs.)
YES
NO
28.ARE YOU NOW OR HAVE YOU EVER BEEN AFFILIATED WITH ANY ORGANIZATION OR MOVEMENT THAT SEEKS TO ALTER OUR FORM OF GOVERNMENT BY UNCONSTITUTIONAL MEANS, OR SYMPATHETICALLY ASSOCIATED WITH ANY SUCH ORGANIZATION, MOVEMENT, OR MEMBERS THEREOF?
YES
NO (If yes, please describe.)
29.ARE THERE ANY OTHER UNFAVORABLE INCIDENTS IN YOUR LIFE WHICH YOU BELIEVE MAY REFLECT UPON YOUR LOYALTY TO THE UNITED STATES GOVERNMENT OR UPON YOUR ABILITY TO PERFORM THE DUTIES WHICH YOU MAY BE CALLED UPON TO UNDERTAKE?
YES
NO (If yes, please describe.)
30.HEALTH CARE PRACTITIONERS AND JUDGE ADVOCATE APPLICANTS ONLY
A. LIST ALL STATE OR FEDERAL BAR LICENSES HELD CURRENTLY OR AT ANY TIME IN THE PAST
STATE IN WHICH LICENSED
DATE LICENSED
EXPIRATION DATE
STATE IN WHICH LICENSED
DATE LICENSED
EXPIRATION DATE
B. APPLICANT MUST INITIAL EACH QUESTION
(1) HAVE YOU EVER HAD ANY OF THE ABOVE STATE LICENSE(S) SUSPENDED OR REVOKED?
(Initials) |
|
YES |
|
NO (If yes, please explain in "REMARKS.") |
(2) HAVE YOU EVER VOLUNTARILY SURRENDERED OR FAILED TO RENEW ANY OF THE ABOVE STATE LICENSES?
(Initials) |
|
YES |
|
|
|
NO (If yes, please explain in "REMARKS.")
(3)HAVE YOU EVER HAD ANY MEDICAL CLAIMS, SETTLEMENTS, JUDICIAL, OR ADMINISTRATIVE ADJUDICATION, OR GRIEVANCES, OR ANY OTHER RESOLVED OR OPEN CHARGES OF INAPPROPRIATE, UNETHICAL, UNPROFESSIONAL, OR SUBSTANDARD MEDICAL CARE OR LEGAL MALPRACTICE?
(Initials) |
|
YES |
NO (If yes, please explain in "REMARKS.")
(4)HAVE YOU EVER HAD YOUR PROFESSIONAL PRIVILEGES WITHDRAWN, DENIED, OR RESTRICTED BY ANY HEALTH CARE INSTITUTION OR STATE BAR LICENSING ORGANIZATION, OR HAVE YOU EVER VOLUNTARILY SURRENDERED YOUR PRIVILEGES?
(Initials) |
|
YES |
|
NO (If yes, please explain in "REMARKS.") |
|
|
|
|
|
|
|
|
|
|
(5) ARE YOU BOARD CERTIFIED? |
|
|
|
|
(Initials) |
|
YES |
|
NO (If no, please explain in "REMARKS.") |
|
|
|||
|
|
|
|
|
|
|
|
|
|
(6) ARE YOU BOARD ELIGIBLE? |
|
|
|
|
(Initials) |
|
YES |
|
NO (If no, please explain in "REMARKS.") |
|
|
(7) HAVE YOU EVER TAKEN THE WRITTEN AND/OR ORAL PORTION OF YOUR BOARD OR BAR EXAMINATION AND FAILED?
(Initials) |
|
YES |
|
|
|
NO (If yes, please explain in "REMARKS.")
(8) DO YOU PLAN TO TAKE OR RETAKE YOUR BOARDS OR BAR EXAMINATION IN THE FUTURE?
(Initials) |
|
YES |
|
|
|
|
|
NO (If yes, when? |
please explain in "REMARKS.") |
31. AFOQT SCORES (Only AFTCOs or Unit Commanders are authorized to enter scores)
AFOQT FORM
DATE TESTED
PILOT
NAV TECH
AA
VERBAL
QUANTITATIVE
32. SECURITY CLEARANCE (X as applicable)
NONE |
|
PENDING: DATE INITIATED (YYYYMMDD) |
|
GRANTED: TYPE: |
DATE GRANTED |
33.REMARKS (If additional space is needed, continue on page 4. Be sure to identify item number.)
I understand that any false or incomplete information knowingly provided on or with this application may be grounds for not employing or accessing with the Air Force, or grounds for dismissing or releasing me from active duty if already employed or serving.
NAME (First, Full Middle, Last Name) (Typed or Printed)
SIGNATURE (First, Full Middle, and Last Name)
DATE
AF FORM 24, 20100622 |
PREVIOUS EDITIONS ARE OBSOLETE |
PAGE 3 OF 4 PAGES |
ADDITIONAL COMMENTS OR EXPLANATIONS
ITEM
NO.
IDENTIFY THE ITEM NUMBER AND EXPLAIN IN THIS SPACE(If additional space is required, use full sheets of paper. Write your name and SSN on each sheet.)
1."I have read and understand HQ USAFRS FS _______________________________ (initial)
2.Short Notice Orders
"I have been briefed on and understand the following":
a. Shipment of household goods is dependent upon receipt of my active duty orders and availability of a common carrier arranged through a local military Traffic Management Office (TMO). _________________ (initial)
b.If I receive my active duty orders less than 30 days from entering active duty, I may not be able to ship household goods prior to my departure for training at Maxwell/Gunter Air Force Base, Alabama, or my permanent duty station. If this causes undue hardship, I understand that a change to my reporting date may be requested _________________ (initial)
c.Should I need to return to my current residence to ship household goods or pickup Family Members, I will be responsible for any travel expenses above those associated with traveling from Maxwell/Gunter Air Force Base, Alabama, to my permanent duty station. Also, any additional time taken over authorized travel time will be charged as leave _________________ (initial)
AF FORM 24, 20100622 |
PREVIOUS EDITIONS ARE OBSOLETE. |
PAGE 4 OF 4 PAGES |
AF FORM 24 CONTINUATION SHEET
AF FORM 24, 20100622 |
PREVIOUS EDITIONS ARE OBSOLETE |