
af component health online can be completed online with ease. Simply make use of FormsPal PDF tool to get it done right away. The tool is continually updated by our team, acquiring cool features and becoming greater. Getting underway is easy! All you should do is follow the next basic steps directly below:
Step 1: First of all, open the pdf editor by clicking the "Get Form Button" in the top section of this webpage.
Step 2: As soon as you start the online editor, you will find the document prepared to be completed. Other than filling in various blanks, you may as well perform some other things with the PDF, that is writing your own textual content, changing the initial text, inserting graphics, signing the PDF, and more.
It really is an easy task to complete the form with our practical tutorial! Here's what you must do:
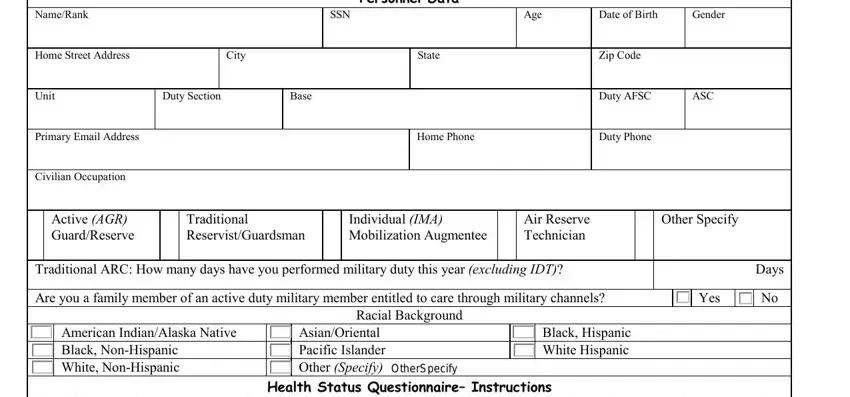
1. The af component health online needs specific information to be inserted. Ensure that the following blanks are completed:
2. Once your current task is complete, take the next step – fill out all of these fields - Mark the appropriate response to, Overall SelfAssessment of Health, Excellent, Very Good, Good, Fair, Poor, Are you on a renewable flying or, Do you have any allergies to, Yes, Yes, AF FORM EFV, and Page with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
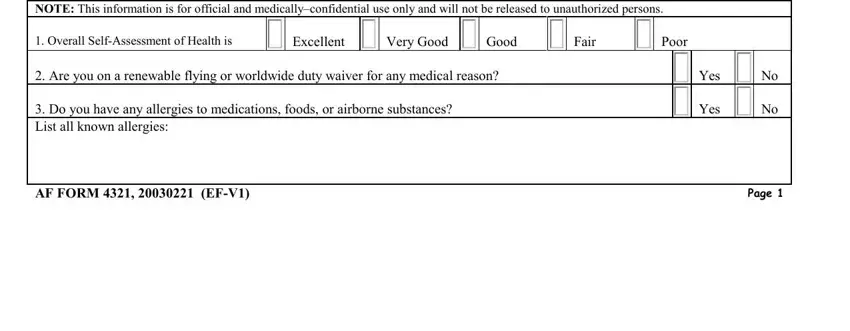
As for Poor and AF FORM EFV, make certain you get them right in this section. Those two are viewed as the most significant fields in this PDF.
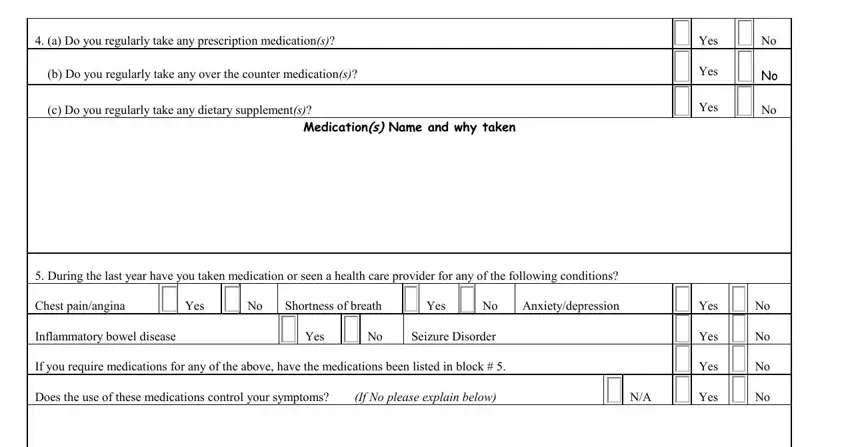
3. This 3rd step is considered quite uncomplicated, a Do you regularly take any, b Do you regularly take any over, c Do you regularly take any, Medications Name and why taken, During the last year have you, Chest painangina, Yes, Shortness of breath, Yes, Anxietydepression, Inflammatory bowel disease, Yes, Seizure Disorder, If you require medications for any, and Does the use of these medications - every one of these empty fields has to be filled in here.
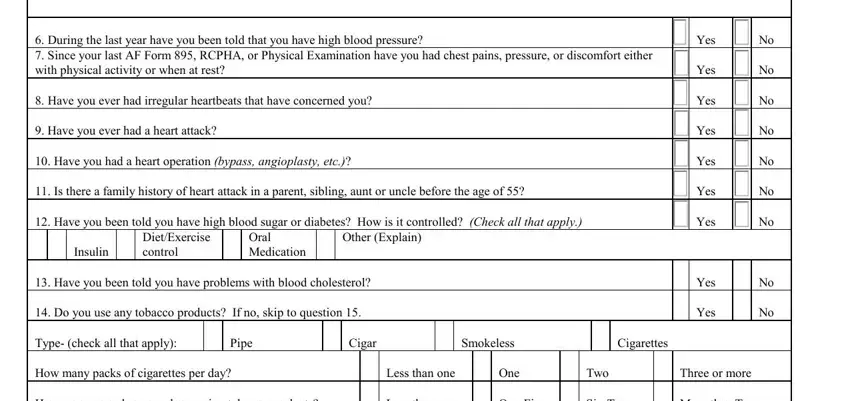
4. This paragraph comes next with all of the following empty form fields to type in your particulars in: During the last year have you, Have you had a heart operation, Is there a family history of, Have you been told you have high, Insulin, DietExercise control, Oral Medication, Other Explain, Have you been told you have, Do you use any tobacco products, Yes, Yes, Yes, Yes, and Yes.
5. Finally, the following final subsection is precisely what you will need to wrap up prior to using the document. The blank fields under consideration are the next: Date, NameRank, SSN, Do you ever experience shortness, Have you ever been told you have, Do you engage in a program of, Light Exercise, Moderate Exercise, Heavy Exercise, Do you have a physical condition, Has your treating physician, Do you have any bone joint or, Are you on any medications for, a Do you consume alcoholic, and Yes.
Step 3: After you have looked over the details in the document, press "Done" to finalize your form. Join us now and easily access af component health online, ready for download. Every single change you make is conveniently preserved , which enables you to change the form later on when necessary. FormsPal ensures your data confidentiality by using a protected system that never saves or distributes any kind of personal information involved in the process. Be confident knowing your paperwork are kept safe each time you work with our service!