
Dealing with PDF documents online is always super easy with our PDF editor. Anyone can fill out request alabama pharmacy here effortlessly. Our editor is constantly evolving to grant the very best user experience attainable, and that is thanks to our dedication to constant enhancement and listening closely to customer comments. Getting underway is simple! Everything you need to do is take the following basic steps down below:
Step 1: Just click on the "Get Form Button" at the top of this site to start up our pdf form editing tool. Here you will find all that is required to work with your document.
Step 2: The tool offers the capability to work with PDF forms in a range of ways. Change it with your own text, correct what's originally in the file, and include a signature - all when you need it!
Pay attention while completing this form. Make certain all required blanks are done correctly.
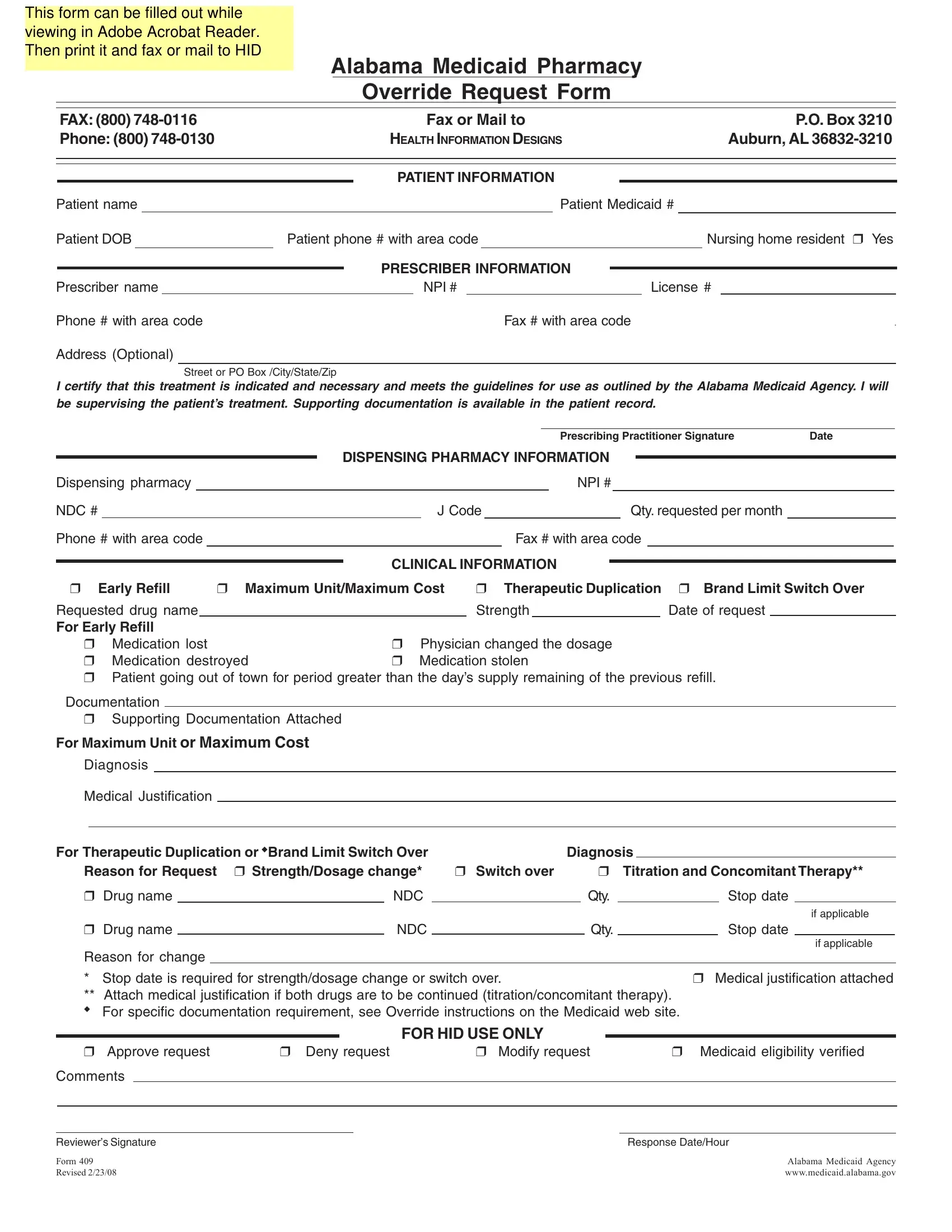
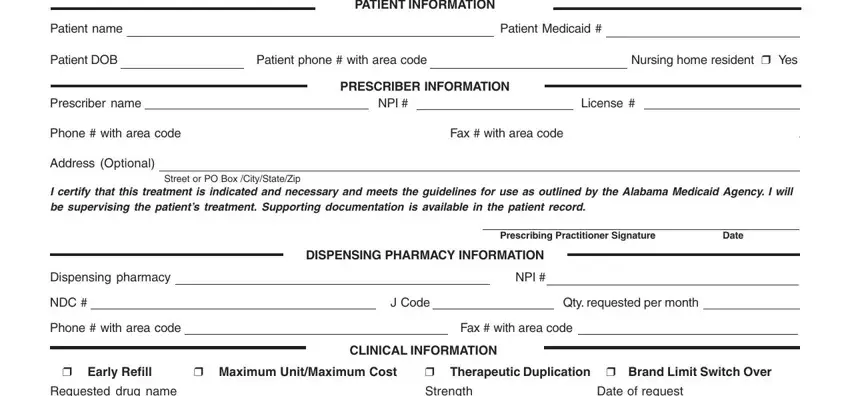
1. You need to complete the request alabama pharmacy properly, hence be careful when filling out the segments that contain all of these fields:
2. The next stage is usually to submit these particular fields: Requested drug name For Early, Strength, Date of request, Medication lost Medication, Physician changed the dosage , Documentation, Supporting Documentation Attached, For Maximum Unit or Maximum Cost, Diagnosis, Medical Justification, For Therapeutic Duplication or, Diagnosis, Switch over, Titration and Concomitant Therapy, and Drug name.
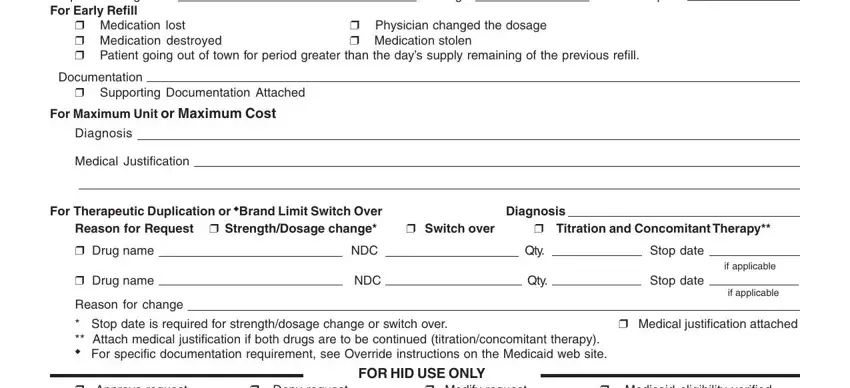
Be very careful while filling in Titration and Concomitant Therapy and Switch over, because this is where most users make some mistakes.
3. The next part is going to be hassle-free - fill out all of the form fields in Approve request, Deny request, Modify request, Medicaid eligibility verified, Comments, Reviewers Signature, Form Revised , Response DateHour, and Alabama Medicaid Agency to complete this process.

Step 3: Always make sure that your details are right and then click "Done" to finish the process. After creating a7-day free trial account here, you'll be able to download request alabama pharmacy or email it immediately. The form will also be available from your personal account menu with your every edit. We do not share or sell any information you use whenever working with documents at our website.