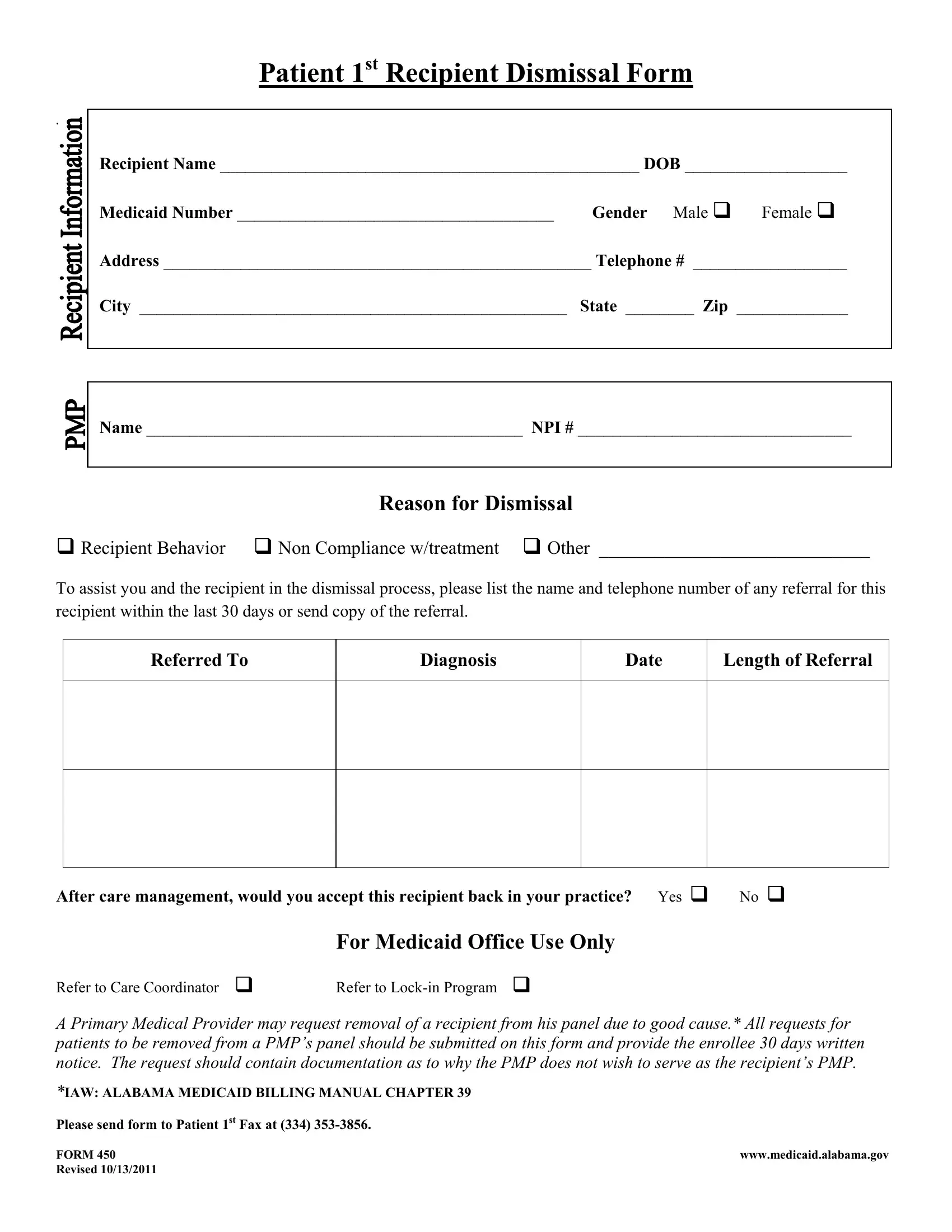
Navigating the complexities of Medicaid in Alabama can be challenging, especially when it comes to understanding specific forms like the Alabama 450 form, also known as the Patient 1st Recipient Dismissal Form. This particular form plays a critical role in the management and administration of care for Medicaid recipients. It is specifically designed for use by Primary Medical Providers (PMPs) who find themselves needing to request the removal of a patient from their panel for reasons deemed to be of good cause. Such reasons may include recipient behavior, non-compliance with treatment, or other factors that make it unfeasible for the provider to continue offering care to the recipient. The form requires detailed information about the recipient, including their name, date of birth, Medicaid number, gender, contact information, and the reason for dismissal. Moreover, it outlines the process for referring the dismissed recipient to another healthcare provider, ensuring that the recipient's care is not unduly disrupted. This process includes providing the name and contact information of the new provider, along with details of any recent referrals. Additionally, the form inquires whether the PMP would be willing to reaccept the recipient back into their practice in the future, underlining the Alabama Medicaid program's commitment to flexibility and patient care. The completion and submission of this form to the appropriate Medicaid office, along with adherence to specified guidelines such as giving a 30-day written notice to the enrollee, underline the formal and structured process that governs patient dismissal and care continuity in the Alabama Medicaid system.
| Question | Answer |
|---|---|
| Form Name | Alabama Form 450 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | enrollee, recipients, Medicaid, ALABAMA |
Patient 1st Recipient Dismissal Form
.
Recipient Name _________________________________________________ DOB ___________________
Medicaid Number _____________________________________ Gender Male Female
Address __________________________________________________ Telephone # __________________
City __________________________________________________ State ________ Zip _____________
Name ____________________________________________ NPI # ________________________________
Reason for Dismissal
Recipient Behavior Non Compliance w/treatment Other _____________________________
To assist you and the recipient in the dismissal process, please list the name and telephone number of any referral for this recipient within the last 30 days or send copy of the referral.
Referred To
Diagnosis
Date
Length of Referral
After care management, would you accept this recipient back in your practice? Yes No
|
For Medicaid Office Use Only |
Refer to Care Coordinator |
Refer to |
A Primary Medical Provider may request removal of a recipient from his panel due to good cause.* All requests for patients to be removed from a PMP’s panel should be submitted on this form and provide the enrollee 30 days written notice. The request should contain documentation as to why the PMP does not wish to serve as the recipient’s PMP.
*IAW: ALABAMA MEDICAID BILLING MANUAL CHAPTER 39
Please send form to Patient 1st Fax at (334)
FORM 450 |
www.medicaid.alabama.gov |
Revised 10/13/2011 |
|