2/23/12
Instructions for Completing
The Alabama Medicaid Agency Referral Form (Form 362)
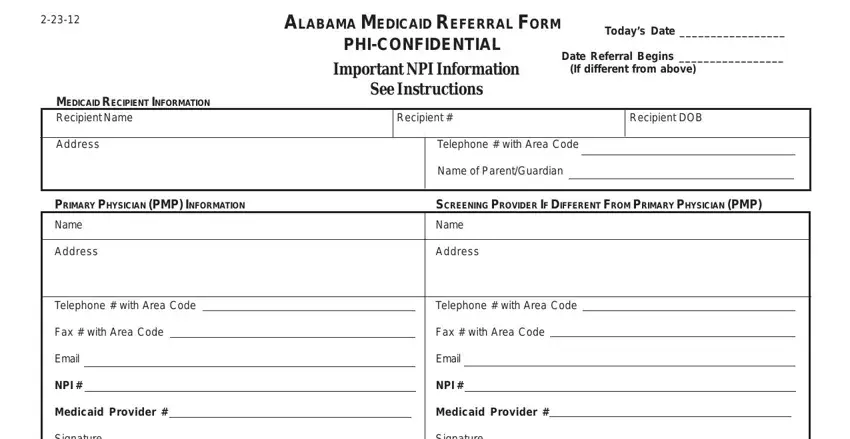
TODAY’S DATE: Date form completed
REFERRAL DATE: Date referral becomes effective
RECIPIENT INFORMATION:
Patient’s name, Medicaid number, date of birth, address, telephone number and parent’s/guardian’s name
PRIMARY PHYSICIAN:* Provide all PMP information. For hard copy referrals, the printed, typed, or stamped name of the primary care physicians with an original signature of the physician or designee is required. Stamped or copied signatures will not be accepted. For electronic referrals provider certification is made via standardized electronic signature protocol.
SCREENING PROVIDER:* Screening provider (if different from primary physician) must complete and sign if the referral is the result of an EPSDT screening.
*NPI INFORMATION: Provide NPI number. For billing purposes indicate Medicaid Provider number, if available.
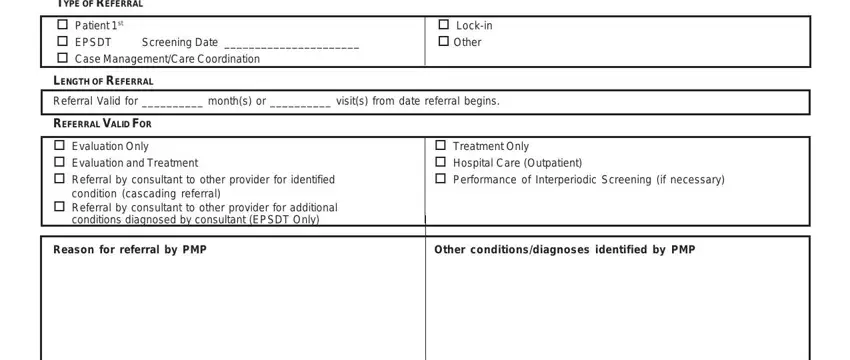
TYPE OF REFERRAL:
◆Patient 1st - Referral to consultant for Patient 1st recipient only (See *Chapter 39 for Claim Filing Instructions).
◆EPSDT - Referral resulting from an EPSDT screening of a child not in the Patient 1st program - indicate screening date (See *Appendix A for Claim Filing Instructions).
◆Case Management/Care Coordination - Referral for case management services through Patient 1st
Care Coordinators (See *Chapter 39 for Claim Filing Instructions).
◆Lock-In - Referral for recipients on lock-in status who are locked in to one doctor and/or one pharmacy (See *Chapter 3 -3.3.2 for Claim Filing Instructions).
◆Patient 1st/EPSDT - Referral is a result of an EPSDT screening of a child who is in the Patient 1st program - indicate screening date (See *Appendix A for Claim Filing Instructions).
◆Other - For recipients who are not in Patient 1st program.
LENGTH OF REFERRAL: Indicate the number of visits/length of time for which the referral is valid.
Note: Must be completed for the referral to be valid.
REFERRAL VALID FOR:
◆Evaluation Only - Consultant will evaluate and provide findings to Primary Physician (PMP).
◆Evaluation and Treatment - Consultant can evaluate and treat for diagnosis listed on the referral.
♦Referral by Consultant to Other Provider For Identified Condition (Cascading Referral) - After evaluation, consultant may, using
Primary Physician’s (PMP) provider number, refer recipient to another specialist as indicated for the condition identified on the referral form.
◆Referral by Consultant To Other Provider For Additional Conditions Diagnosed By Consultant (Cascading Referral) - Consultant may refer recipient to another specialist for other diagnosed conditions without having to get an additional referral from
the Primary Physician (PMP).
◆Treatment Only - Consultant will treat for diagnosis listed on referral.
◆Hospital Care (Outpatient) - Consultant may provide care in an outpatient setting.
◆Performance of Interperiodic Screening (if necessary) - Consultant may perform an interperiodic screening if a condition was diagnosed that will require continued care or future follow-up visits.
REASON FOR REFERRAL BY PRIMARY PHYSICIAN (PMP):
Indicate the reason/condition the recipient is being referred.
OTHER CONDITIONS/DIAGNOSIS IDENTIFIED BY PRIMARY PHYSICIAN:
Indicate any condition present at the time of initial exam by PMP.
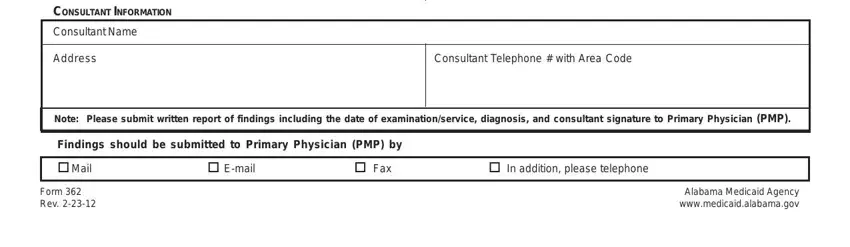
CONSULTANT INFORMATION: Consultant’s name, address and telephone number.
PLEASE SUBMIT FINDINGS TO PRIMARY PHYSICIAN BY: The Primary Physician (PMP) should indicate how he/she wants to be notified by the consultant of findings and/or treatment rendered.
*The Alabama Medicaid Provider Manual is available on the Alabama Medicaid website| at http://www.medicaid.alabama.gov/CONTENT/6.0_Providers/6.7_Manuals.aspx
2-23-12 |
|
|
|
|
ALABAMA MEDICAID REFERRAL FORM |
|
|
Today’s Date _________________ |
|
|
|
|
|
|
|
|
|
|
|
|
PHI-CONFIDENTIAL |
Date Referral Begins _________________ |
|
|
|
|
|
Important NPI Information |
|
|
|
|
|
|
(If different from above) |
MEDICAID RECIPIENT INFORMATION |
See Instructions |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Recipient Name |
|
|
|
|
Recipient # |
|
|
|
Recipient DOB |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address |
|
|
|
|
|
|
|
Telephone # with Area Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name of Parent/Guardian |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PRIMARY PHYSICIAN (PMP) INFORMATION |
|
|
|
|
SCREENING PROVIDER IF DIFFERENT FROM PRIMARY PHYSICIAN (PMP) |
Name |
|
|
|
|
|
|
|
Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address |
|
|
|
|
|
|
|
Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Telephone # with Area Code |
|
|
|
|
|
Telephone # with Area Code |
|
|
Fax # with Area Code |
|
|
|
|
|
Fax # with Area Code |
|
|
|
|
|
|
|
|
|
Email |
|
|
|
|
|
|
|
|
Email |
|
|
|
|
|
|
|
|
|
NPI # |
|
|
|
|
|
|
|
|
NPI # |
|
|
|
|
|
|
|
|
|
Medicaid Provider # |
|
|
|
|
|
Medicaid Provider # |
|
|
|
|
|
|
|
|
|
Signature |
|
|
|
|
|
|
|
Signature |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TYPE OF REFERRAL |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Patient 1st |
|
|
|
|
|
|
|
Lock-in |
|
|
|
|
|
|
|
|
EPSDT |
Screening Date ______________________ |
|
|
|
|
Other |
|
|
|
|
|
|
|
|
Case Management/Care Coordination |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LENGTH OF REFERRAL |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Referral Valid for __________ month(s) or __________ visit(s) from date referral begins. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
REFERRAL VALID FOR |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Evaluation Only |
|
|
|
|
Treatment Only |
|
|
|
|
|
|
|
|
Evaluation and Treatment |
|
|
|
|
Hospital Care (Outpatient) |
Referral by consultant to other provider for identified |
|
|
|
|
Performance of Interperiodic Screening (if necessary) |
condition (cascading referral)
Referral by consultant to other provider for additional conditions diagnosed by consultant (EPSDT Only)
Reason for referral by PMP |
Other conditions/diagnoses identified by PMP |
CONSULTANT INFORMATION
Consultant Name
Address
Consultant Telephone # with Area Code
Note: Please submit written report of findings including the date of examination/service, diagnosis, and consultant signature to Primary Physician (PMP).
Findings should be submitted to Primary Physician (PMP) by
Mail |
E-mail |
Fax |
In addition, please telephone |
Form 362 |
Alabama Medicaid Agency |
Rev. 2-23-12 |
www.medicaid.alabama.gov |