
How to Fill Out the Allstate Wellness Claim Application Form
Follow these steps to complete your Allstate Wellness Claim Application correctly and avoid processing delays.
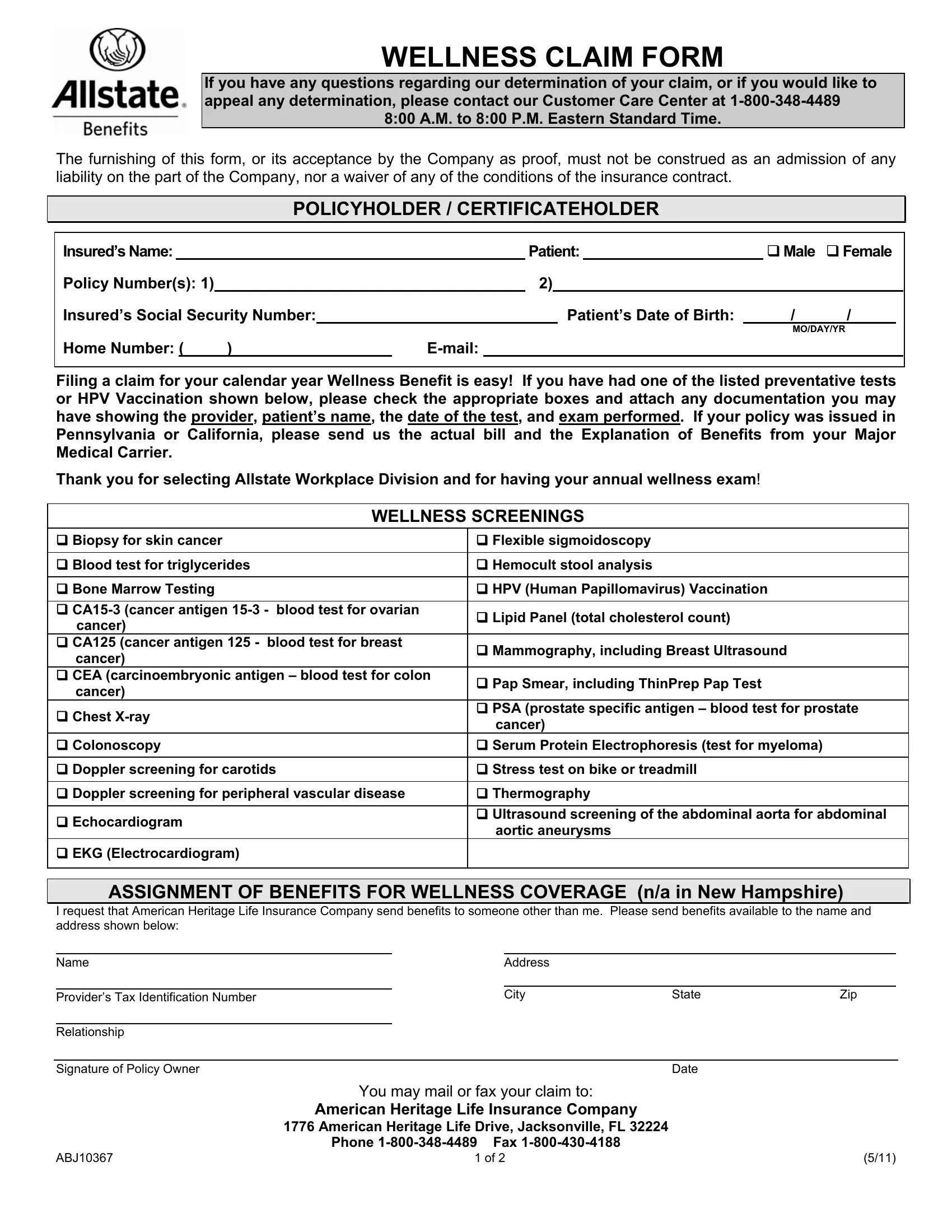
- Gather required information. Before you begin, collect your Allstate policy number(s), your social security number, the patient's full name and date of birth, and the date each wellness service was performed.
- Complete the insured information section. Enter the primary policyholder's name, address, and contact details in the top section of the form.
- List wellness services received. In the claim section, check each preventative test or screening you received during the benefit year. Covered services include mammograms, blood tests for cancer markers, echocardiograms, stress tests, and HPV vaccinations.
- Complete the assignment of benefits (optional). If you want your benefit paid directly to a healthcare provider, complete this section. Note that this option is not available in New Hampshire.
- Sign the authorization section. Read the authorization and sign the form. Your signature allows Allstate to obtain medical records needed to review your claim.
- Attach supporting documentation. Include copies of Explanation of Benefits (EOB) statements, receipts, or laboratory reports for each service claimed. Original documents are not required.
- Mail the completed form. Send the signed form and supporting documents to the address printed on your Allstate policy. Keep a copy for your records.
What Wellness Benefits Are Covered?
The Allstate Wellness Claim Application covers a range of annual preventative services under most Allstate wellness benefit riders. Covered screenings typically include blood pressure checks, cholesterol panels, blood glucose tests, mammograms, Pap smears, prostate-specific antigen (PSA) tests, colonoscopies, and the HPV vaccination series.
Coverage details and reimbursement amounts depend on your specific Allstate policy. Review your policy documents or call the number on your policy card to confirm which services qualify before submitting your wellness claim.
Frequently Asked Questions
How long does it take to process an Allstate wellness claim?
Processing times vary, but most wellness claims are reviewed within 30 days of receipt. If Allstate needs additional information, they will contact you at the address on file.
Can I submit the Allstate Wellness Claim Application electronically?
The standard form is a paper-based PDF. You can fill it out digitally using FormsPal, then print and mail the completed form. Check your current policy documents for any electronic submission options offered through the MyBenefits portal.
What documentation should I attach to my wellness claim?
Attach copies of your EOB statements, itemized bills, or lab reports for each service. If you received the HPV vaccination, include a copy of the vaccine record or receipt from your healthcare provider.
Is there a deadline to file an Allstate wellness benefit claim?
Most Allstate wellness benefit riders require claims to be submitted within 90 days of the end of the benefit year. Check your policy for the exact filing deadline.
Related Insurance Claim Forms
- Allstate Appeal Form – use this to dispute a denied claim or request a benefit review
- Allstate Critical Illness Form – for filing a critical illness benefit claim under your Allstate policy
- Health Insurance Claim Form – a general health insurance claim form for use with various carriers
- AARP Claim Form – for AARP life insurance benefit claims