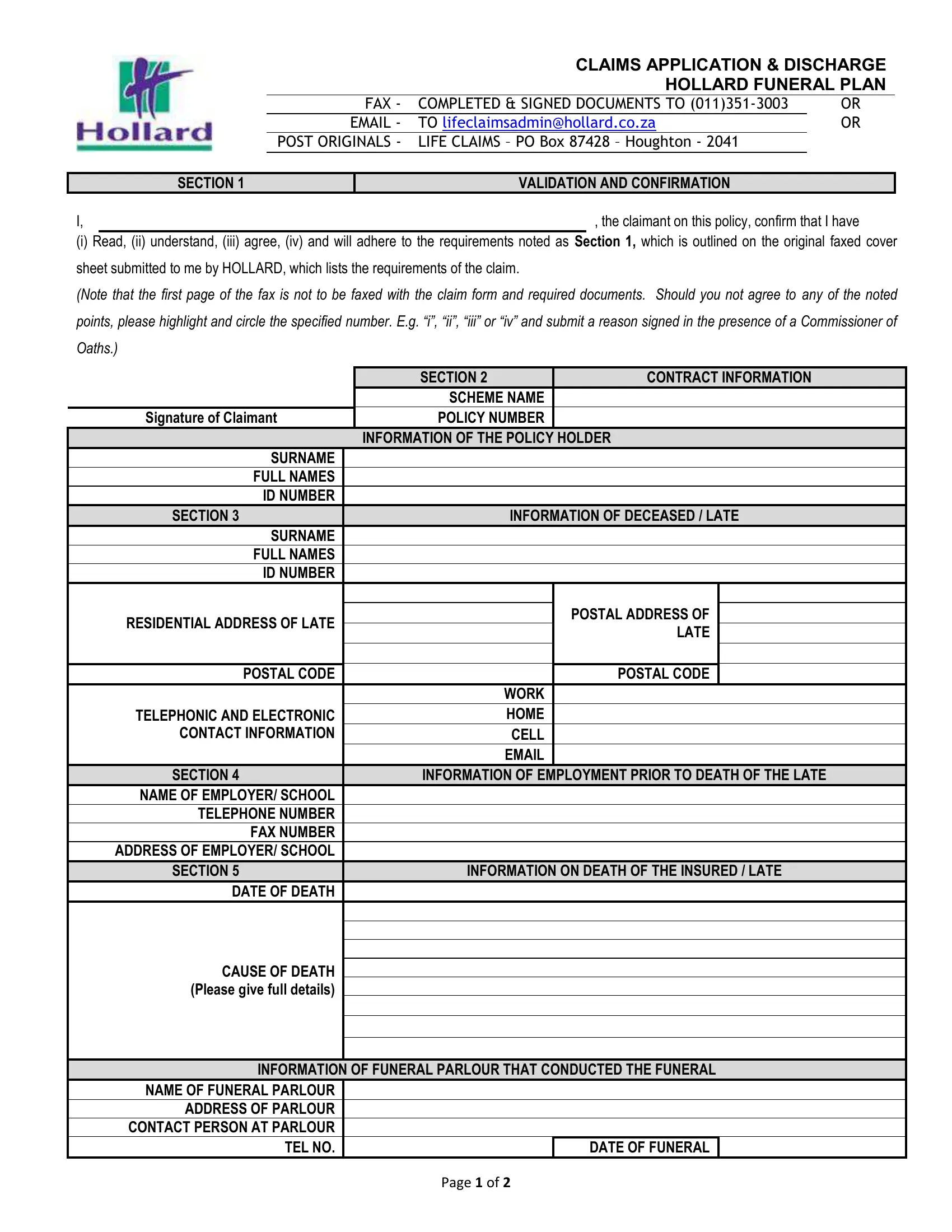
The Claim Application Discharge Hollard form helps claimants navigate the funeral plan claim process during a difficult time. It guides you through all required sections, from verifying your identity as the authorized claimant to providing full details about the policyholder and the deceased.
The form covers employment details of the deceased prior to death, the circumstances of death, and the specifics of the funeral service. It also details the method of transferring the claim payment to the claimant, ensuring that all necessary financial information is communicated accurately. Each section is clearly labeled to make completion straightforward, even without legal assistance.
A consent section allows Hollard to access and verify sensitive personal information with relevant third parties such as government databases. This step is required for all Hollard funeral plan claims and ensures that the payout reaches the correct beneficiary without delays. The form also includes a tribal authority section for claimants who fall under traditional community leadership structures.
Completing the Claim Application Discharge Hollard form correctly on the first submission helps avoid processing delays. Common reasons for delays include missing signatures, incorrect bank account details, and incomplete information about the deceased's employment history. Gathering all required documents before starting the form will save time and reduce the risk of rejection.
| Question | Answer |
|---|---|
| Form Name | Claim Application Discharge Hollard Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | funeral form for work, burial society membership form, bi 1663 form no download needed, bi 1663 form sample |