
Should you desire to fill out ambetter inpatient prior authorization fax form, it's not necessary to download and install any sort of software - just try our PDF editor. Our tool is consistently developing to deliver the very best user experience possible, and that is thanks to our resolve for constant development and listening closely to testimonials. To begin your journey, go through these simple steps:
Step 1: Click on the "Get Form" button in the top area of this webpage to get into our PDF editor.
Step 2: This editor provides you with the ability to work with nearly all PDF files in various ways. Transform it by adding your own text, adjust existing content, and put in a signature - all close at hand!
This PDF form will require particular information to be entered, thus you should definitely take the time to fill in what is asked:
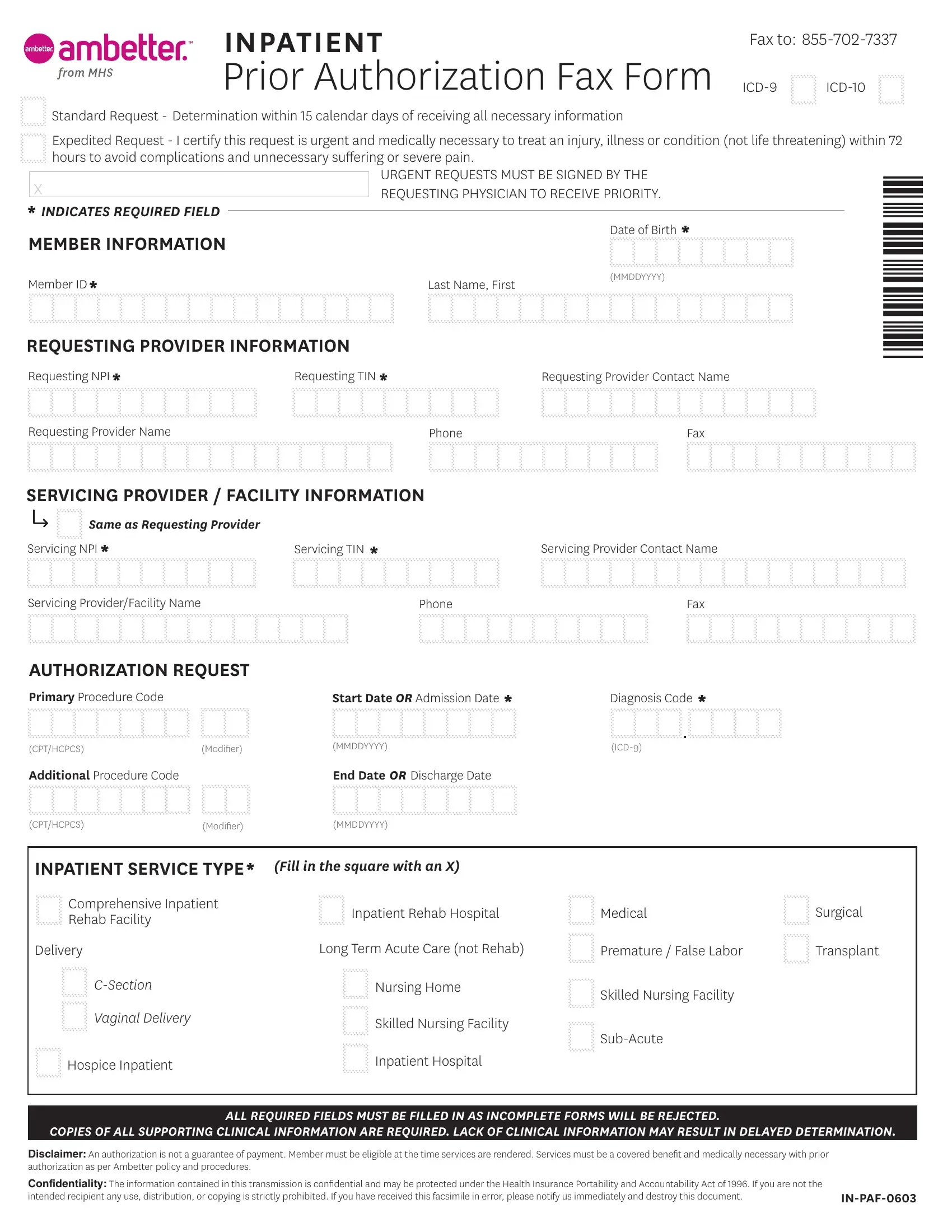
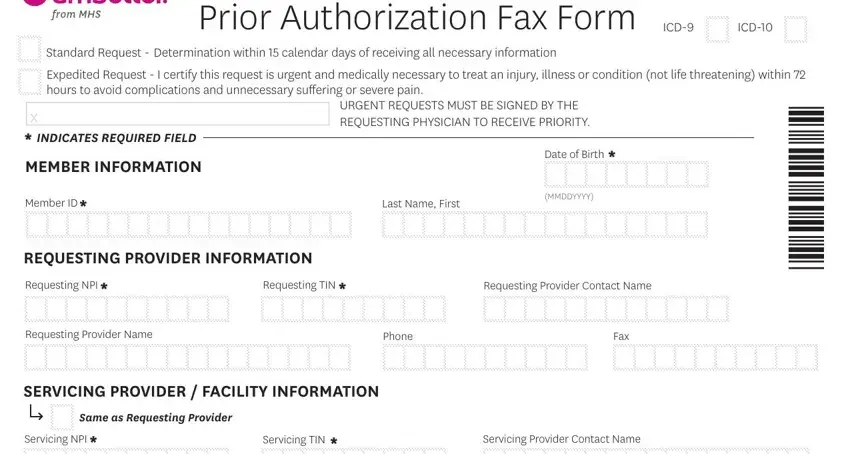
1. Fill out your ambetter inpatient prior authorization fax form with a group of major blanks. Collect all of the necessary information and make sure nothing is overlooked!
2. Given that the previous array of fields is done, you have to put in the required specifics in Servicing ProviderFacility Name, Phone, Fax, AUTHORIZATION REQUEST, Primary Procedure Code, Start Date OR Admission Date , Diagnosis Code , CPTHCPCS, Modiier, MMDDYYYY, ICD, Additional Procedure Code, End Date OR Discharge Date, CPTHCPCS, and Modiier so you're able to move on further.
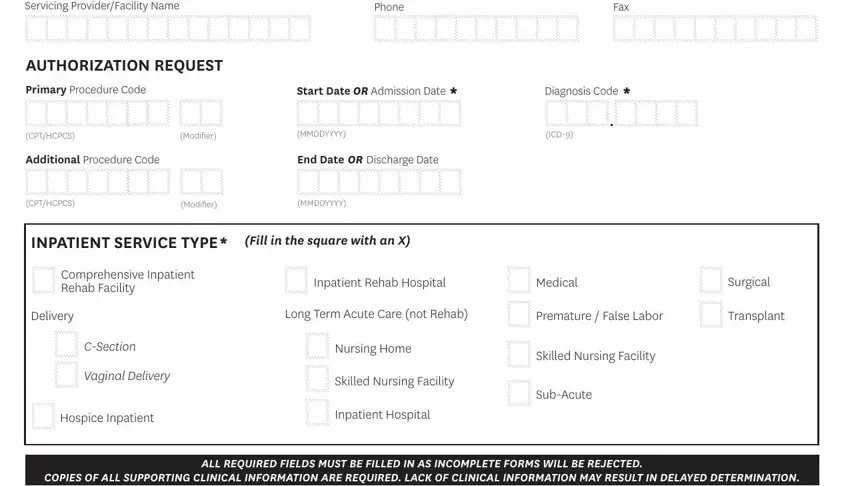
Always be really attentive while filling out CPTHCPCS and Diagnosis Code , since this is where many people make errors.
Step 3: Prior to moving on, you should make sure that blank fields have been filled in right. Once you are satisfied with it, click “Done." Sign up with FormsPal right now and instantly use ambetter inpatient prior authorization fax form, ready for download. All modifications you make are kept , meaning you can change the document at a later time if required. We don't sell or share the details that you provide whenever completing documents at FormsPal.