With the objective of allowing it to be as effortless to apply as possible, we developed our PDF editor. The process of filling in the ambetter authorization is going to be hassle-free in case you stick to the following actions.
Step 1: Initially, press the orange button "Get Form Now".
Step 2: Right now, you can begin modifying the ambetter authorization. Our multifunctional toolbar is readily available - insert, delete, modify, highlight, and undertake similar commands with the content material in the file.
These particular areas will compose the PDF file that you will be filling in:
Note the appropriate information in Servicing NPI, Servicing TIN, Servicing Provider Contact Name, Servicing ProviderFacility Name, Phone, Fax, AUTHORIZATION REQUEST, Primary Procedure Code, Additional Procedure Code, Start Date OR Admission Date, Diagnosis Code, CPTHCPCS, Modifier, CPTHCPCS, and Modifier area.
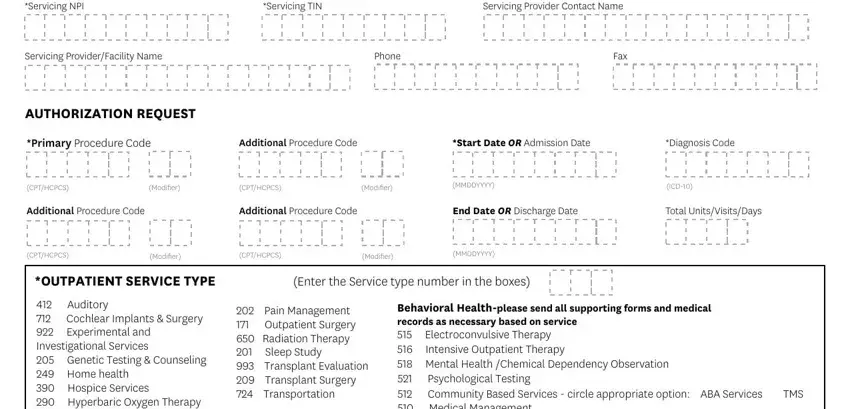
You will need to put down some information within the area Auditory Cochlear Implants, DME Rental Purchase, Purchase Price, Behavioral Healthplease send all, ALL REQUIRED FIELDS MUST BE FILLED, Disclaimer An authorization is not, and Rev EWPAF.
Step 3: Select the Done button to save your form. Now it is accessible for export to your gadget.
Step 4: You can generate duplicates of your form toavoid all possible problems. You need not worry, we don't share or track your data.
