
 LMP
LMPOur PDF editor makes it simple to complete Anthem Form 151 online without printing or mailing a paper copy. Follow the steps below to fill out the form and save your completed document.
Step 1: Open the Form
Click the "Get Form Here" button at the top of this page. The form will load in the online PDF editor, ready for you to begin entering information.
Step 2: Enter Provider and Member Information
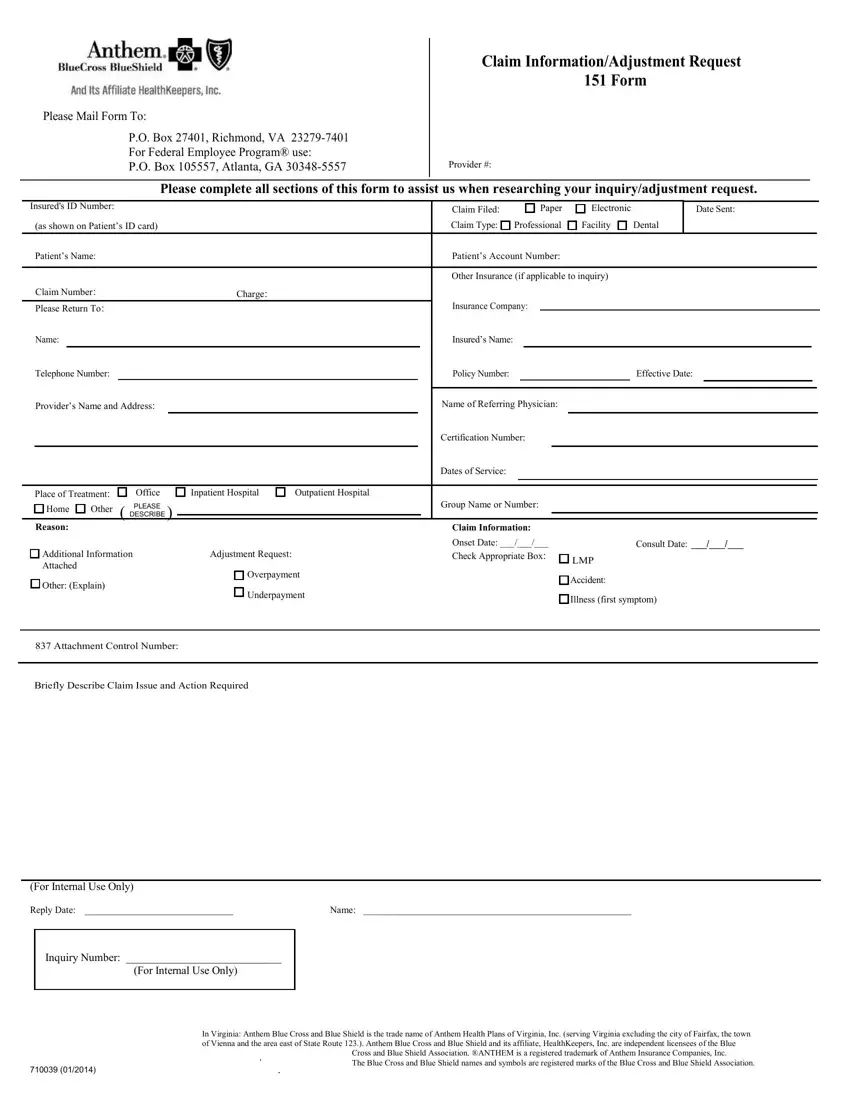
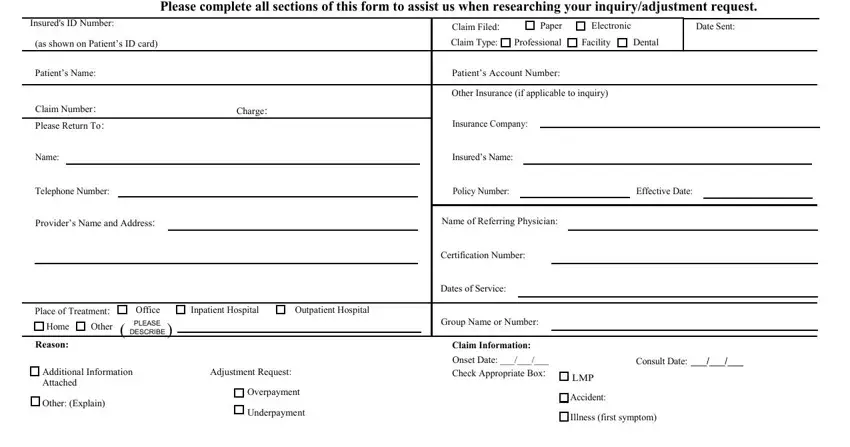
Fill in the provider's name, address, and National Provider Identifier (NPI). Then enter the insured member's name and Anthem identification number. These fields appear at the top of the form and must be completed before moving on to the claim details section.
Step 3: Complete the Claim Detail Fields
In the claim details section, enter the original claim number, the date of service, the amount billed, and the amount that Anthem paid. Select the type of claim (professional services, facility, or dental) and whether the original submission was paper or electronic. In the section labeled "For Internal Use Only," fill in the Reply Date, Name, and Inquiry Number as prompted.
Step 4: Describe the Issue and Action Required
Use the description field to explain the nature of the adjustment. State whether you are reporting an overpayment, an underpayment, or another billing discrepancy. Include the dollar amount in question and the reason for the adjustment request. A clear, specific description reduces the chance that Anthem will need to follow up for additional documentation.
Step 5: Save and Submit
Click the "Done" button to save your completed form. You can download the PDF to your device or print it directly. Mail the completed form to the appropriate Anthem address for your plan type. For Federal Employee Program (FEP) claims, use the FEP-specific mailing address printed on the form.
Step 6: Keep a Copy
Save a copy of the completed form and record the date you mailed it. Anthem typically acknowledges adjustment requests within 30 days. Your information is never shared or tracked by this platform.
