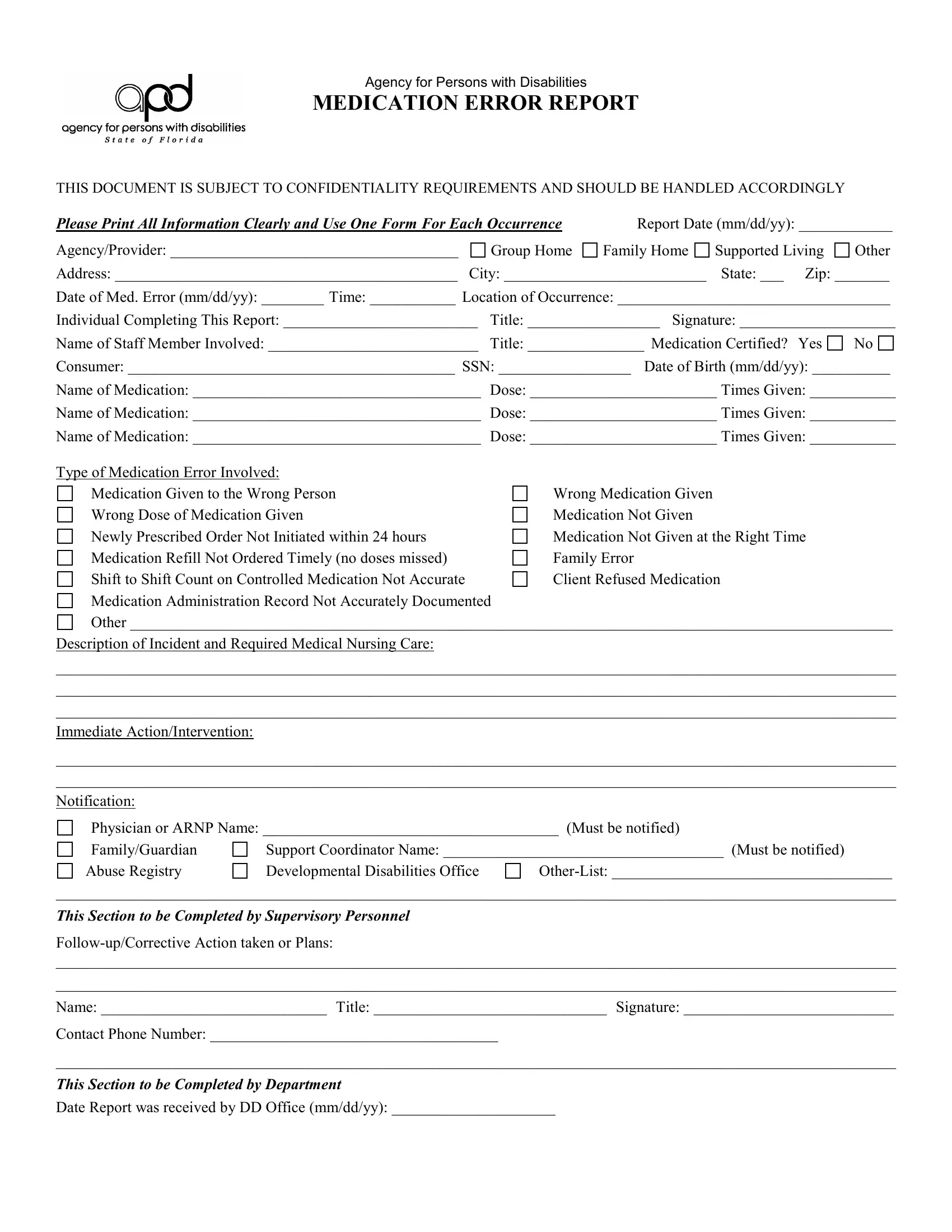
When it comes to ensuring the safety and well-being of individuals with disabilities, meticulous attention to medication management is paramount. The Apd Medication Error form, developed by the Agency for Persons with Disabilities, plays a critical role in this endeavor by providing a structured means to report medication-related errors. This highly confidential document requires thorough completion for each incident, capturing details such as the date and time of the error, the location, and the individuals involved, including both the person completing the report and the staff member associated with the error. Information about the consumer affected, alongside specifics of the medication(s) involved—namely the name, dose, and times administeredis—are equally vital components of the report. The form categorizes the type of medication errors, encompassing a wide range of potential mishaps, from administering medication to the wrong person to delays in medication refills. Further sections of the form demand an in-depth description of the incident, immediate actions taken in response, notifications issued to relevant parties (including physicians and family or guardians), and follow-up or corrective actions planned or executed by supervisory personnel. Lastly, a separate section for the Department to document receipt and recommendations underscores the collaborative effort between direct care providers and supervisory authorities to enhance medication management practices, aiming to mitigate risks and elevate the standard of care offered to individuals with disabilities.
| Question | Answer |
|---|---|
| Form Name | Apd Medication Error Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | agency persons disabilities medication, apd med error report form fillable 2019, agency medication error, apdmyflorida com medication error |
Agency for Persons with Disabilities
MEDICATION ERROR REPORT
THIS DOCUMENT IS SUBJECT TO CONFIDENTIALITY REQUIREMENTS AND SHOULD BE HANDLED ACCORDINGLY
Please Print All Information Clearly and Use One Form For Each Occurrence |
Report Date (mm/dd/yy): ____________ |
|||
Agency/Provider: _____________________________________ |
Group Home |
Family Home |
Supported Living |
Other |
Address: ____________________________________________ |
City: __________________________ |
State: ___ Zip: _______ |
||
Date of Med. Error (mm/dd/yy): ________ Time: ___________ Location of Occurrence: ___________________________________
Individual Completing This Report: _________________________ |
Title: _________________ Signature: ____________________ |
|
Name of Staff Member Involved: ___________________________ |
Title: _______________ Medication Certified? Yes |
No |
Consumer: __________________________________________ SSN: _________________ Date of Birth (mm/dd/yy): __________
Name of Medication: _____________________________________ |
Dose: ________________________ Times Given: ___________ |
Name of Medication: _____________________________________ |
Dose: ________________________ Times Given: ___________ |
Name of Medication: _____________________________________ |
Dose: ________________________ Times Given: ___________ |
Type of Medication Error Involved: |
|
Medication Given to the Wrong Person |
Wrong Medication Given |
Wrong Dose of Medication Given |
Medication Not Given |
Newly Prescribed Order Not Initiated within 24 hours |
Medication Not Given at the Right Time |
Medication Refill Not Ordered Timely (no doses missed) |
Family Error |
Shift to Shift Count on Controlled Medication Not Accurate |
Client Refused Medication |
Medication Administration Record Not Accurately Documented |
|
Other __________________________________________________________________________________________________
Description of Incident and Required Medical Nursing Care:
____________________________________________________________________________________________________________
____________________________________________________________________________________________________________
____________________________________________________________________________________________________________
Immediate Action/Intervention:
____________________________________________________________________________________________________________
____________________________________________________________________________________________________________
Notification:
Physician or ARNP Name: ______________________________________ (Must be notified)
Family/Guardian |
Support Coordinator Name: ____________________________________ (Must be notified) |
|
Abuse Registry |
Developmental Disabilities Office |
|
____________________________________________________________________________________________________________
This Section to be Completed by Supervisory Personnel
____________________________________________________________________________________________________________
____________________________________________________________________________________________________________
Name: _____________________________ Title: ______________________________ Signature: ___________________________
Contact Phone Number: _____________________________________
____________________________________________________________________________________________________________
This Section to be Completed by Department
Date Report was received by DD Office (mm/dd/yy): _____________________
____________________________________________________________________________________________________________
____________________________________________________________________________________________________________
APD Form