
Complete the APD Provider Enrollment Application form online using FormsPal's no-cost online PDF editor. Click the link on this page to open your application request, fill it out directly in your browser, and file the finished form at your local area office. Use the download link to save a copy of your request for your records.
How to Fill Out the APD Provider Enrollment Application Form
Step 1: Click the "Get Form" button or use the direct link at the top of this page to open the online editor for your APD provider form.
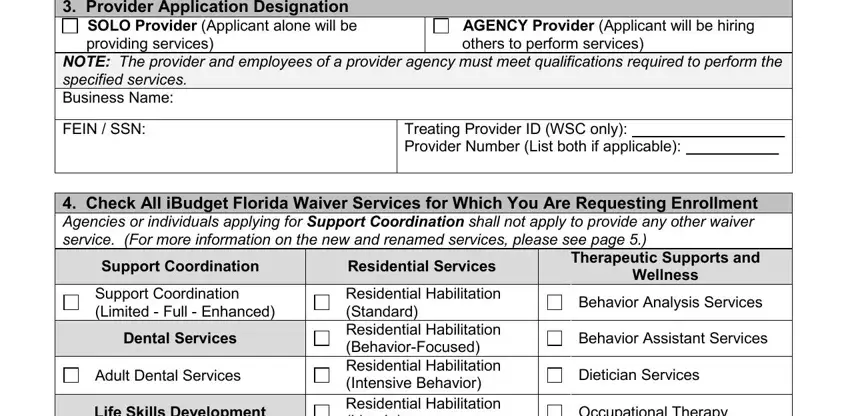
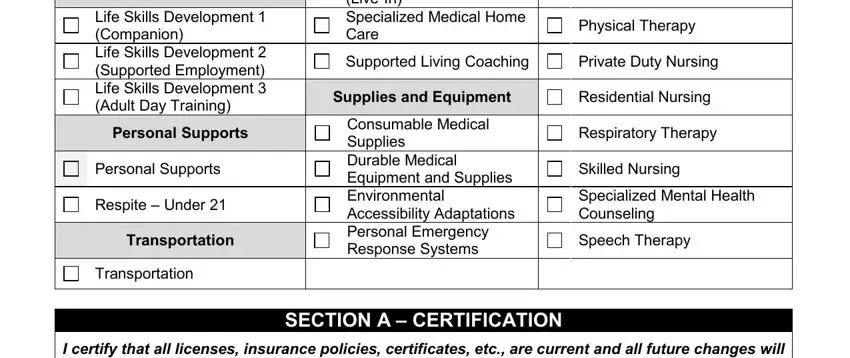
Step 2: In the first part of the application, complete your designation, list all geographic coverage areas, enter your FEIN or SSN, and select the iBudget waiver programs you plan to offer. If you are applying as a support coordinator, include your treating ID number. Agencies must also indicate that they will employ others to deliver care on their behalf. Please note that all individuals applying as solo applicants must complete this part in full.
Step 3: New applicants and agencies adding program types must complete the second part of the form with educational background, degrees obtained, professional qualifications, and license or certification details. Include effective dates and expiration dates for all credentials listed on the application. Learn what documents are required by contacting your local area office before you begin this part.
Step 4: Applicants offering residential habilitation, supported living coaching, or support coordination must include a written plan explaining how they will meet community-based client needs at all hours. Complete the signature and date fields, then file this part of the application at your area office. Please attach all required documents to your request before submission.
Step 5: Review all information before finishing. Confirm your degree, school or college name, date completed, license registration or certification number, expiration date, state licensing authority, and agency details. Click "Done" and create a no-cost account to download the finished APD application form or send it by email. Learn more about the APD community programs on the official state website to confirm your form is complete before you file your request.
APD Provider Enrollment Application - Frequently Asked Questions
Who needs to submit an APD provider application request?
Any agency or individuals seeking to become an APD waiver program participant in Florida must complete and file this request. This applies to first-time applicants and agencies requesting to add new program types to their existing authorization. Please contact the local area office to learn current intake procedures for your community.
Where do I file the finished APD application form?
File the finished form and all required attachments at your local area office. Please contact the area office in your region to confirm the correct mailing address and any additional local requirements before sending your application. Learn the specific filing instructions to avoid delays in processing your request.
What documents must applicants attach to the APD form?
Applicants must attach copies of all current licenses, registrations, and certifications. Residential applicants and supported living coaches must also attach a written 24-hour community care plan. All attached information must be current and complete at the time of filing. The area office may request additional documentation if any information is missing or unclear from your original request.
Can I complete the APD provider application form online?
Yes. Use the no-cost FormsPal PDF editor to complete the entire application in your browser. Click the link above to open the form, fill it out, and download the finished application. Use the download link to save a copy for your records, then file your request at the area office. Please visit the official APD community website to learn about current waiver program enrollment requirements.
Looking for related forms? Find the disabled dependent enrollment application, the ACH payment enrollment form, and the 32BJ enrollment form on FormsPal.