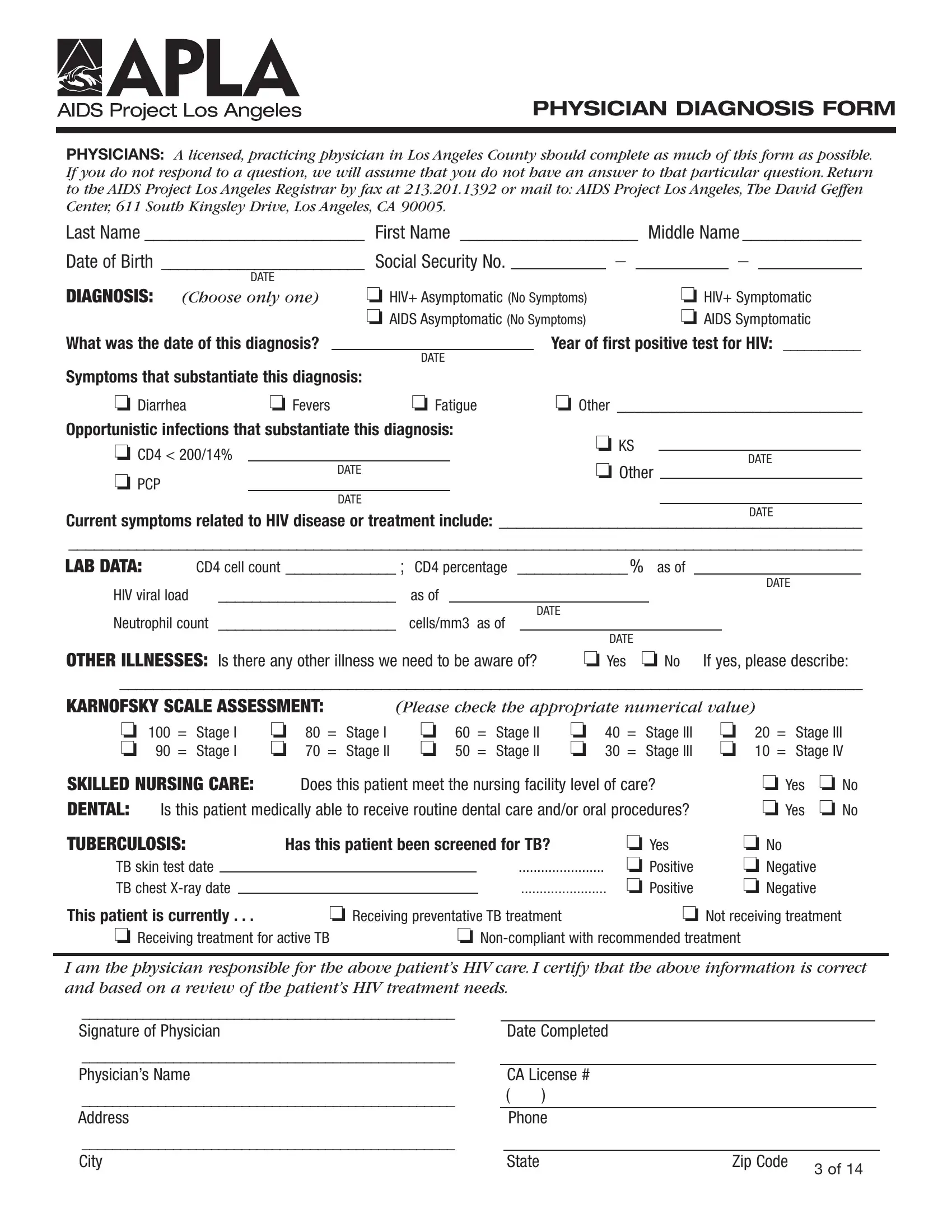

The APLA Diagnosis Form is a one-page document that licensed physicians complete and submit to AIDS Project Los Angeles. Follow the steps below to fill out the form correctly and ensure it meets APLA reporting requirements.
Step 1: Enter Patient Identification Information
Record the patient's full legal name, date of birth, and address at the top of the form. Include any identification or case numbers assigned by APLA or the treating facility. Accurate identification data is required for APLA to match the form to existing patient records.
Step 2: Document the HIV or AIDS Diagnosis Date
Enter the date of the patient's initial HIV diagnosis and, if applicable, the date the condition progressed to AIDS. These dates anchor the patient's care timeline and help APLA determine eligibility for specific support programs.
Step 3: Record Current Symptoms and Opportunistic Infections
List all current symptoms and active opportunistic infections. Common opportunistic infections documented on this form include Pneumocystis pneumonia, toxoplasmosis, and cytomegalovirus. Complete this section as thoroughly as possible to give APLA a full picture of the patient's health status.
Step 4: Enter Laboratory Values
Record the most recent CD4 cell count and HIV viral load from laboratory tests. These values help APLA determine appropriate care levels and connect the patient with the right support resources. Include the date each test was performed.
Step 5: Complete the Karnofsky Scale Assessment
Use the Karnofsky Performance Scale to rate the patient's functional capability. Scores range from 0 to 100, where higher scores indicate greater independent function. This rating helps APLA assess whether the patient requires skilled nursing care or other intensive support services.
Step 6: Address Additional Care Needs
Complete the sections on skilled nursing care requirements, dental health status, and tuberculosis screening results. If TB screening has not been completed, note this on the form. Each of these fields guides APLA's resource allocation decisions for the individual patient.
Step 7: Sign and Submit the Completed Form
The treating physician must sign and date the completed APLA Diagnosis Form. Submit the signed form directly to AIDS Project Los Angeles for processing. APLA reviews each submission to assign care coordinators and direct appropriate community resources to the patient.