Completing this Arizona health coverage application online is straightforward with FormsPal. Our PDF editor is built to help you fill out government forms quickly and accurately. Follow these steps to finish your AHCCCS application:
Step 1: Click the orange "Get Form Now" button to open the form in the online editor.
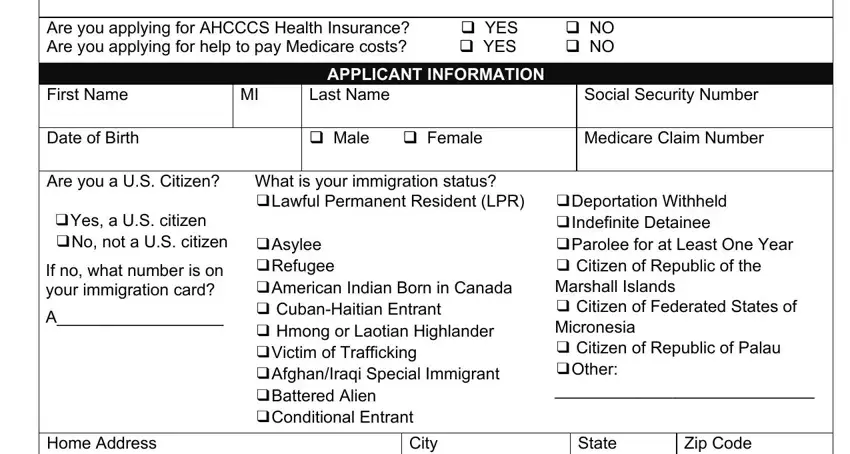
Step 2: Use the toolbar to type, update your information, and fill in each required field. The form collects your personal data, contact details, and health coverage eligibility information.
Enter your details in each section, starting with:
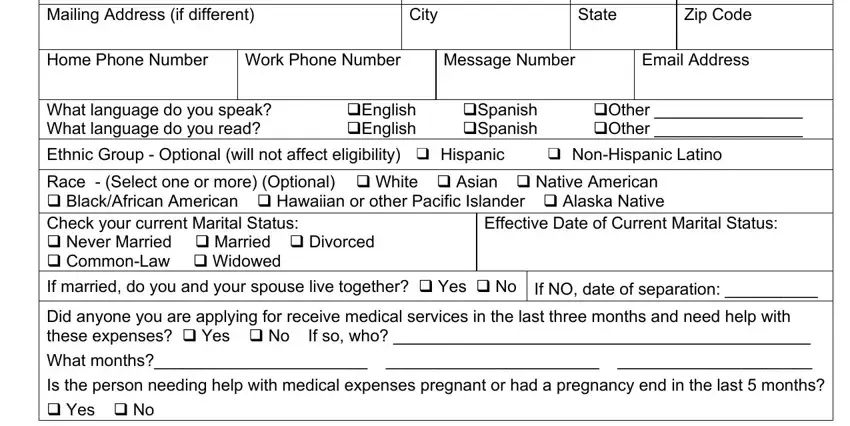
Complete the Mailing Address section, including City, State, Zip Code, Home Phone, Work Phone, and Email Address. Select your preferred language (English or Spanish) and enter the effective date of your current marital status.
Fill in the Authorized Representative section if someone else is helping with your application. Provide their contact details and complete the authorization fields.
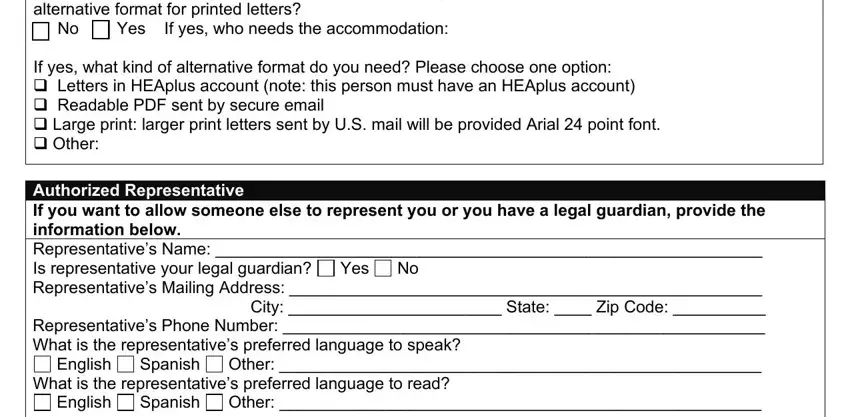
Review the rights and responsibilities section. Indicate your representative preferences and confirm the required contact options.
End by printing the name of the applicant and any authorized representative. Sign and date the form. All signatures are required to complete the document.
Step 3: Click "Done" to save your completed form. You can download it to any device, print it, or send it by email for submission to the Arizona Department of Economic Security.
Step 4: Make two or three printed copies for your records. Keep them in a secure location in case you have questions or need to update your information with AHCCCS later.
Looking for related health coverage forms? See also the health insurance renewal form, Medicaid application form, and Social Security application on FormsPal.
