
You may fill out argos pet insurance claim form online instantly with our online tool for PDF editing. To make our tool better and easier to use, we constantly work on new features, considering suggestions from our users. Here is what you'll want to do to get started:
Step 1: Hit the "Get Form" button above. It is going to open up our pdf editor so that you could start completing your form.
Step 2: This tool offers the capability to work with your PDF form in various ways. Transform it with personalized text, adjust what's originally in the PDF, and include a signature - all when you need it!
As for the fields of this particular form, this is what you should know:
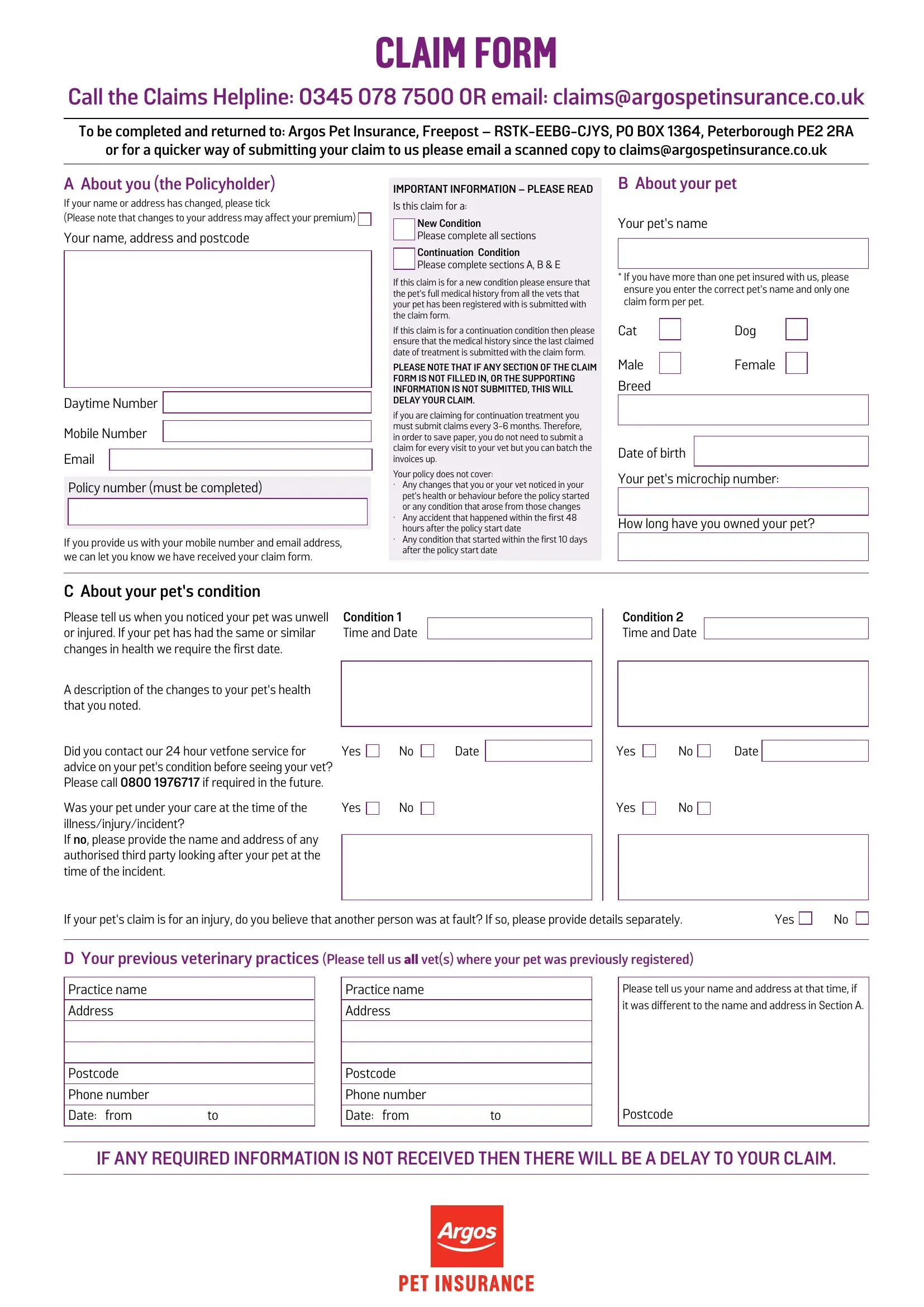
1. The argos pet insurance claim form online requires certain information to be entered. Make certain the subsequent blank fields are finalized:
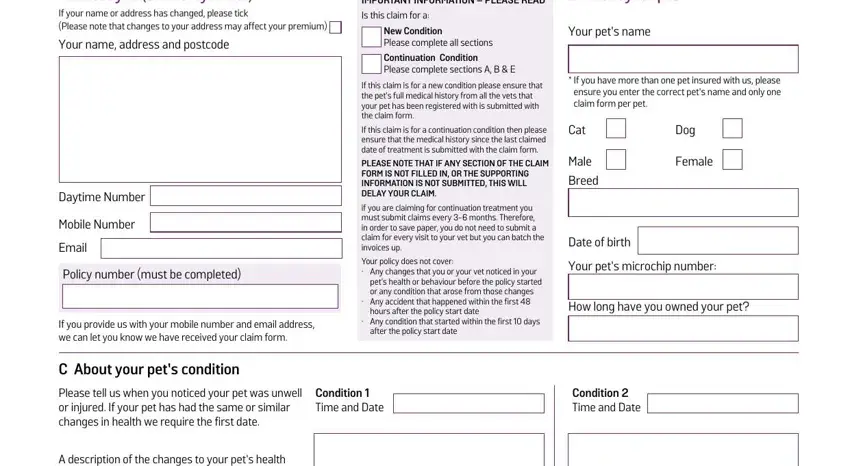
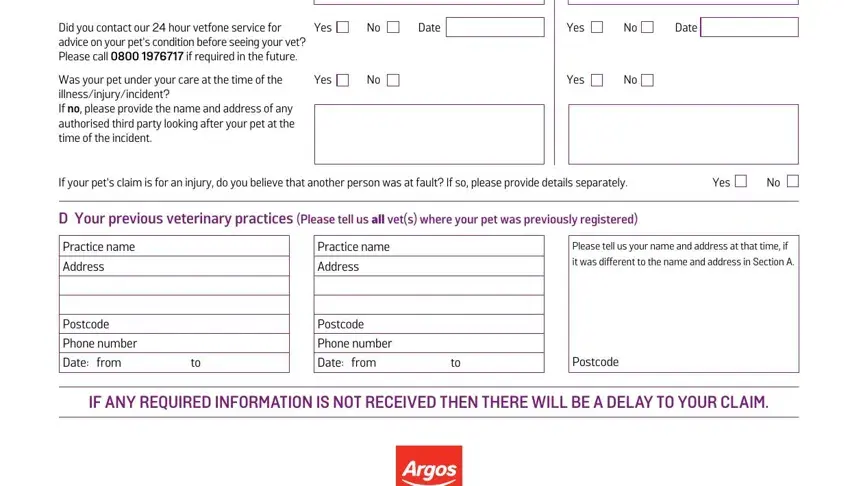
2. Right after filling in this step, go to the subsequent step and enter the necessary particulars in all these blanks - Did you contact our hour vetfone, Was your pet under your care at, Yes, Date, Yes, Date, Yes, Yes, If your pets claim is for an, D Your previous veterinary, Practice name Address, Practice name Address, Please tell us your name and, Postcode Phone number Date from to, and Postcode Phone number Date from to.
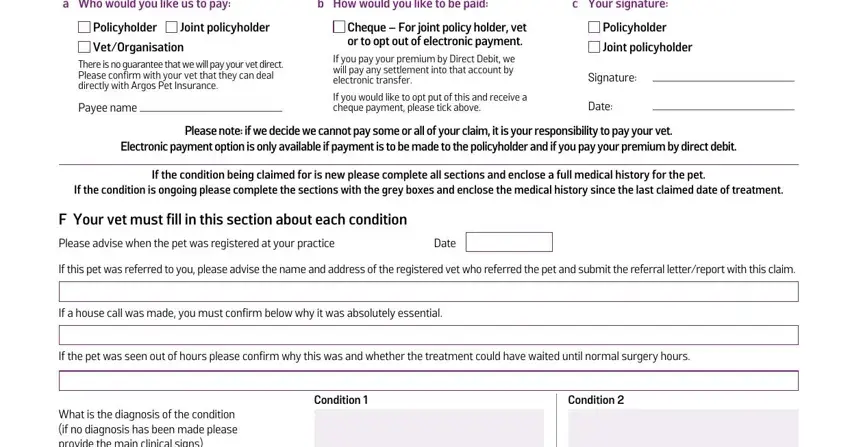
3. Within this stage, have a look at a Who would you like us to pay, b How would you like to be paid, c Your signature, Policyholder VetOrganisation, Joint policyholder, There is no guarantee that we will, Payee name, Cheque For joint policy holder, Policyholder Joint policyholder, Signature, Date, Please note if we decide we cannot, Electronic payment option is only, If the condition being claimed for, and If the condition is ongoing please. Each one of these must be taken care of with highest accuracy.
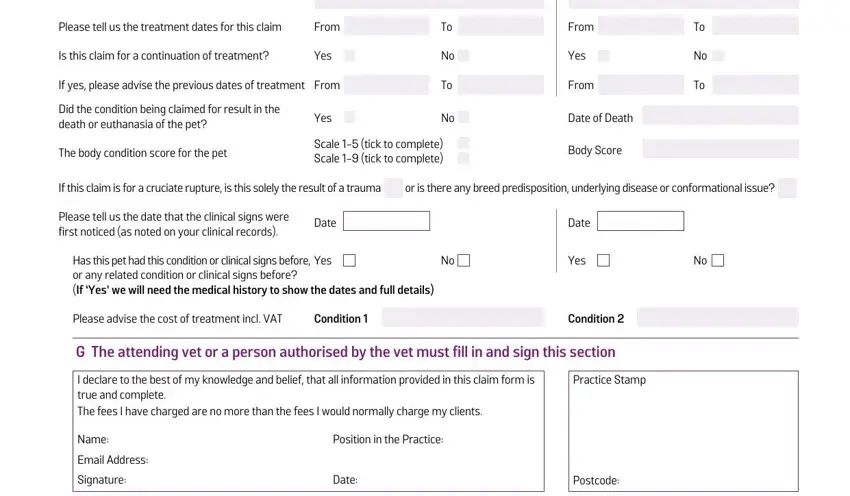
4. The next subsection will require your information in the subsequent areas: Please tell us the treatment dates, From, Is this claim for a continuation, Yes, If yes please advise the previous, Did the condition being claimed, Yes, The body condition score for the, Scale tick to complete Scale , From, Yes, From, Date of Death, Body Score, and If this claim is for a cruciate. Ensure that you fill in all of the required details to go forward.
Always be very mindful while completing Yes and Please tell us the treatment dates, since this is the section where many people make errors.
Step 3: Proofread everything you have entered into the form fields and hit the "Done" button. After getting a7-day free trial account with us, it will be possible to download argos pet insurance claim form online or email it promptly. The PDF file will also be easily accessible in your personal account menu with your every single edit. FormsPal is invested in the confidentiality of all our users; we ensure that all personal data entered into our system continues to be protected.