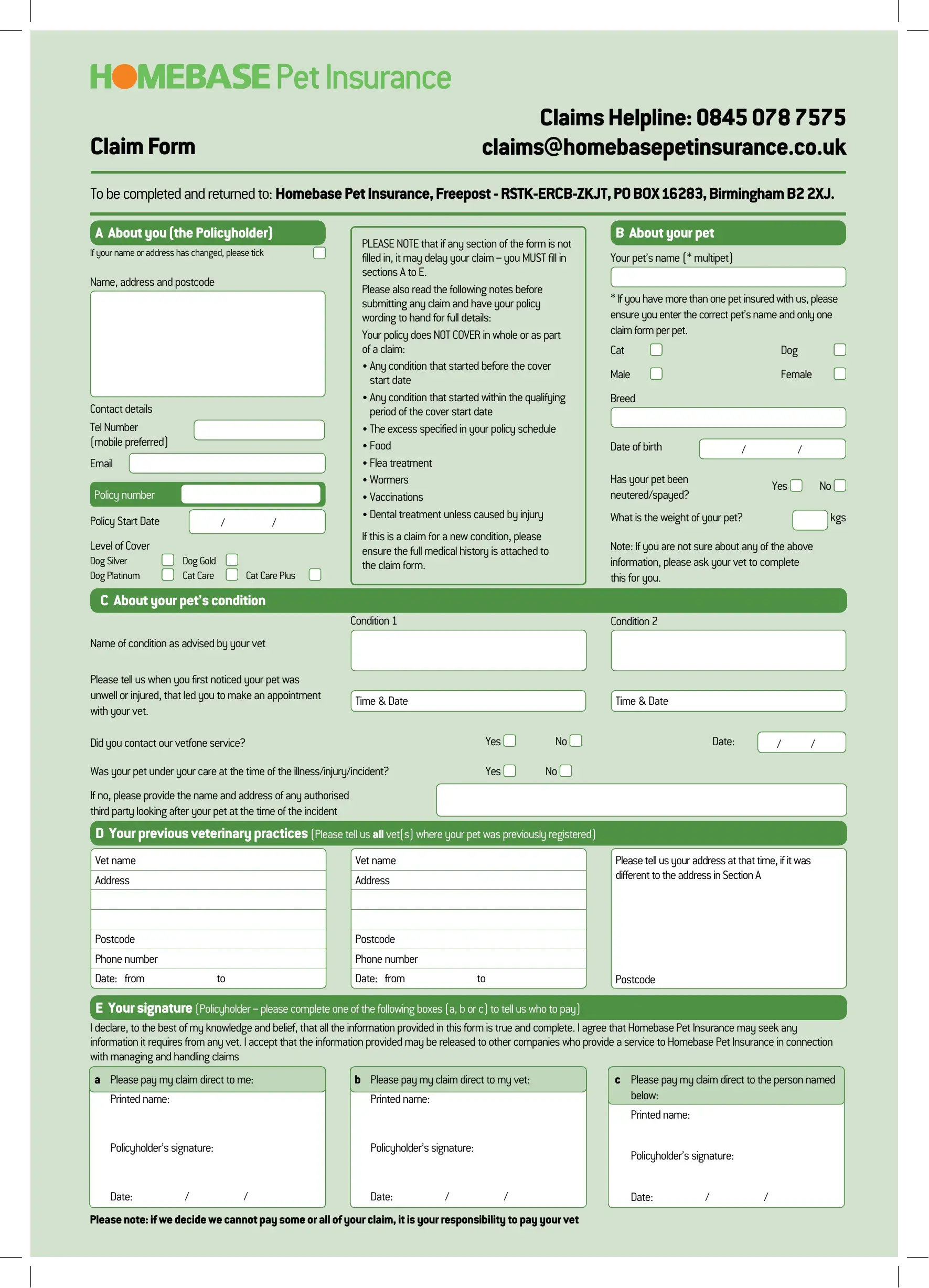
Navigating the maze of insurance claims can often feel overwhelming, especially when it comes to the well-being of our furry friends. The Homebase Pet Insurance Claim Form serves as a crucial first step in this process, inviting policyholders to provide comprehensive details to ensure their pet's health issues are promptly addressed and compensated according to their policy. With sections ranging from basic owner and pet information, detailed accounts of the pet’s condition, previous veterinary practices, to the policyholder’s preferred method of payment, the form is designed to collect all necessary information in a structured manner. It emphasizes the importance of including a pet's full medical history for new conditions and clearly outlines what is not covered, such as pre-existing conditions, certain types of treatments, and the specified excess. Furthermore, the form accommodates claims involving complementary treatments and requires a detailed veterinary declaration to avoid any discrepancies. By completing and returning this form to Homebase Pet Insurance, policyholders take a vital step towards managing their pet's health care needs efficiently, although they are reminded of their responsibility to cover any part of the claim not accepted by the insurer.
| Question | Answer |
|---|---|
| Form Name | Homebase Pet Insurance Claim Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | pets at home claim form pdf, vpi pet insurance claim form, fillable vpi claim, homebase pet insurance claim form |