There isn't anything challenging about completing the medicare authorization disclose once you open our PDF tool. By following these simple steps, you will definitely get the prepared PDF document within the minimum period you can.
Step 1: Click the "Get Form Now" button to begin the process.
Step 2: So, you're on the document editing page. You can add text, edit existing data, highlight particular words or phrases, put crosses or checks, add images, sign the document, erase needless fields, etc.
For each segment, create the information required by the platform.
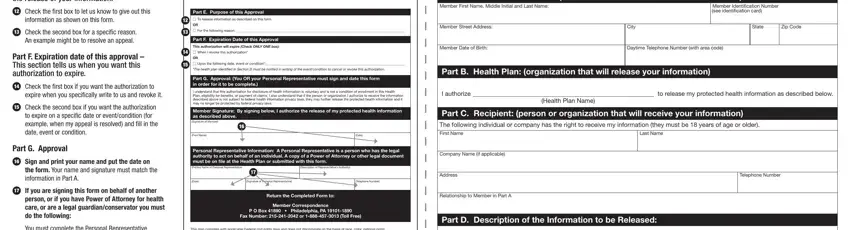
Enter the required details in the box Printed Name of Personal, Description of Representatives, Date, Signature of Personal, Telephone Number, Return the Completed Form to, Member Correspondence P O Box, This plan complies with applicable, ATENCIÓN Si habla español cuenta, Write the full name address, The individual that you designate, part d description of the, For only psychotherapy notes check, For all of your information check, and For only limited information check.
Inside the area dealing with Personal Representative, Printed Name of Personal, Description of Representatives, Date, Signature of Personal, Telephone Number, Company Name if applicable, Address, Telephone Number, part e purpose of this approval, Check the first box to let us know, Check the second box for a, part f expiration date of this, Check the first box if you want, and Check the second box if you want, you will need to put down some demanded details.
The general or durable power of, legal guardianship This is when, Conservatorship This happens when, himherself, executor of estate or death, M Premium billing and payment M, and procedure treatment, M Referral M Pharmacy M Other, I also approve the release of the, M Abortion M Abuse, M Genetic testing M HIV or AIDS M, M Mental health M Sexually, I understand that my, PLEASE KEEP A COPY OF THIS FORM, and E R E H T U C box is the place where both sides can indicate their rights and responsibilities.

Check the sections Personal Representative, Printed Name of Personal, Description of Representatives, Date, Signature of Personal, Telephone Number, Company Name if applicable, Address, Return the Completed Form to, Relationship to Member in Part A, Telephone Number, part e purpose of this approval, Check the first box to let us know, Check the second box for a, and part f expiration date of this and thereafter fill them out.
Step 3: Choose the button "Done". The PDF file is available to be transferred. You can easily upload it to your laptop or email it.
Step 4: Ensure that you keep away from potential issues by making minimally a couple of duplicates of the file.
