You can complete this form online using our free PDF editor. The editor makes it simple to enter text, check boxes, add a signature, and navigate between fields on the Amerigroup Authorization Request form for Ohio Medicaid pharmacy prior authorization.
Step 1: Click the orange "Get Form Now" button at the top of this page.
Step 2: The form editing page will open. You can add text, check boxes, insert a signature, and highlight key fields. Use the toolbar to navigate between sections.
The following sections are included in the PDF form:

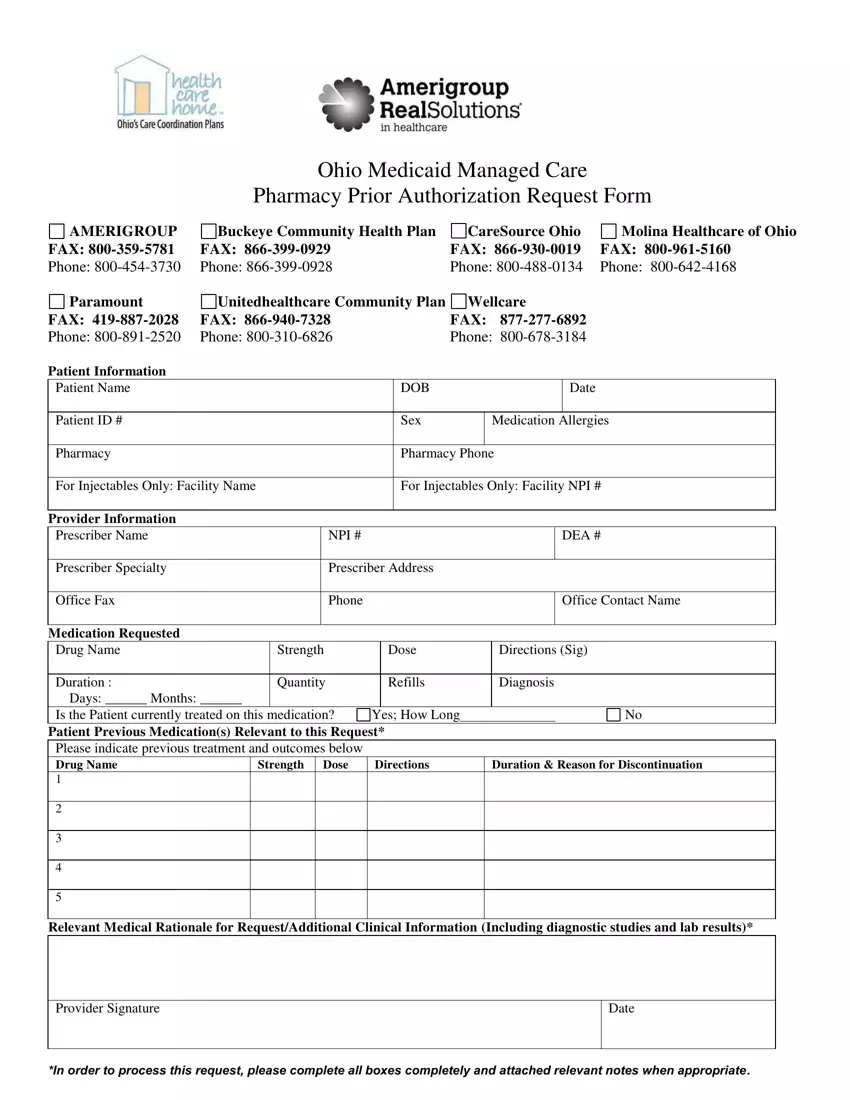
Fill in the Office Fax, Phone, Office Contact Name, Medication Requested, Drug Name, Strength, Dose, Directions, Duration, Quantity, Refills, Diagnosis, previous treatment history, and all other required fields.

Step 3: Click "Done" when all fields are complete. You can download the form, print it, or send it by email directly from the editor.
Step 4: Save extra copies for your records before faxing the completed form to the appropriate managed care plan.
Common Mistakes to Avoid
Missing the member ID or plan name? Always verify the patient's exact plan name before submitting. A mismatch causes the request to be returned unprocessed.
Incomplete clinical rationale? Requests are often denied when the medical rationale section is left short or vague. Include the diagnosis code, prior medications tried, and the reason the requested medication is medically necessary.
Wrong fax number? Each plan listed on the form has a different fax number. Using the wrong one delays processing by several days.
Related Authorization Forms
If you work with other managed care plans or need additional prior authorization forms, these resources may be useful:
