The whole process of completing the bbs is very uncomplicated. We ensured our editor is easy to use and can help fill out just about any document within minutes. Consider the four steps you have to follow:
Step 1: Select the orange button "Get Form Here" on the following page.
Step 2: Now you can edit the bbs. You should use our multifunctional toolbar to include, remove, and adjust the content of the file.
You should enter the next data to be able to fill out the file:
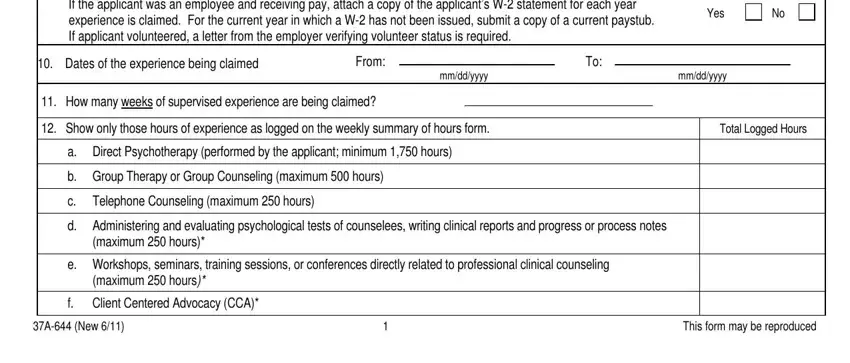
Fill out the If the applicant was an employee, Yes, Dates of the experience being, From, mmddyyyy, mmddyyyy, How many weeks of supervised, Show only those hours of, maximum hours, e Workshops seminars training, maximum hours, f Client Centered Advocacy CCA, Total Logged Hours, A New, and This form may be reproduced space with all the information required by the program.
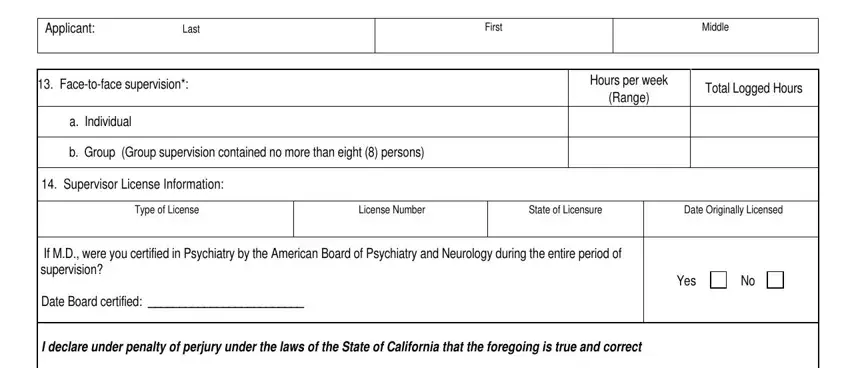
You will have to provide certain information in the segment Applicant, Last, First, Middle, Facetoface supervision, a Individual, b Group Group supervision, Supervisor License Information, Hours per week Range, Total Logged Hours, Type of License, License Number, State of Licensure, Date Originally Licensed, and If MD were you certified in.
Inside of box Signature of Supervisor, Date, and When combined these categories, identify the rights and obligations.
Step 3: As you click on the Done button, the finished document is easily transferable to every of your devices. Or, you can easily deliver it by means of email.
Step 4: Generate copies of your form - it can help you avoid possible future difficulties. And don't worry - we do not share or read your information.
