
24-Hour can be filled in effortlessly. Just use FormsPal PDF editing tool to accomplish the job fast. In order to make our editor better and easier to utilize, we continuously come up with new features, taking into consideration suggestions coming from our users. In case you are seeking to begin, here's what it takes:
Step 1: Press the "Get Form" button at the top of this webpage to get into our editor.
Step 2: When you access the file editor, you'll see the document all set to be completed. Apart from filling in various blank fields, you can also do other sorts of things with the form, such as writing any textual content, modifying the initial text, inserting graphics, signing the form, and more.
It will be an easy task to finish the pdf with our helpful tutorial! This is what you need to do:
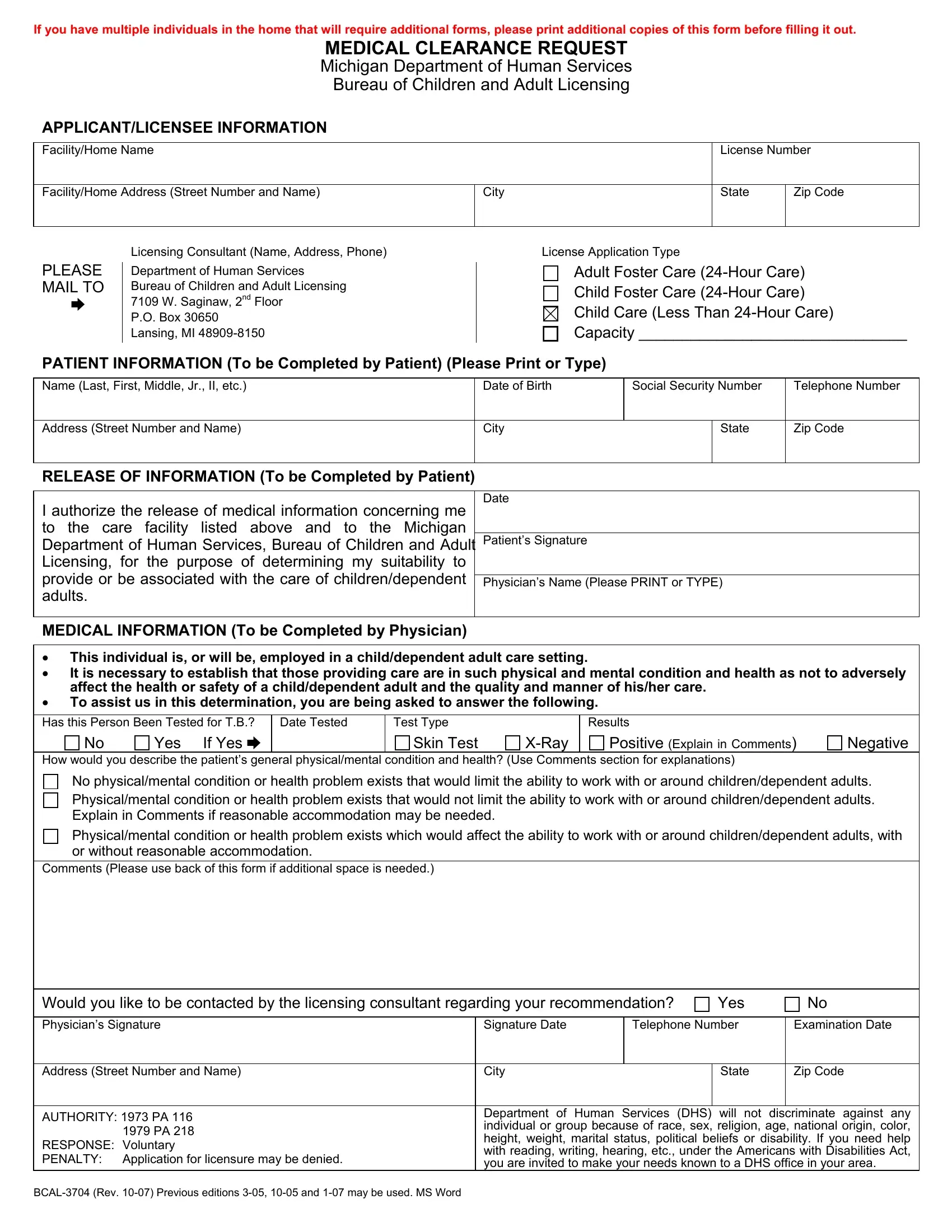
1. While filling in the 24-Hour, be certain to incorporate all necessary blanks within its relevant area. It will help facilitate the work, making it possible for your information to be processed efficiently and properly.
2. Given that the last segment is done, it's time to insert the essential particulars in This individual is or will be, Has this Person Been Tested for TB, Date Tested, Test Type, Results, Yes, If Yes cid, Skin Test, XRay, Positive Explain in Comments, Negative, How would you describe the, No physicalmental condition or, Explain in Comments if reasonable, and Physicalmental condition or health so you're able to progress to the third stage.
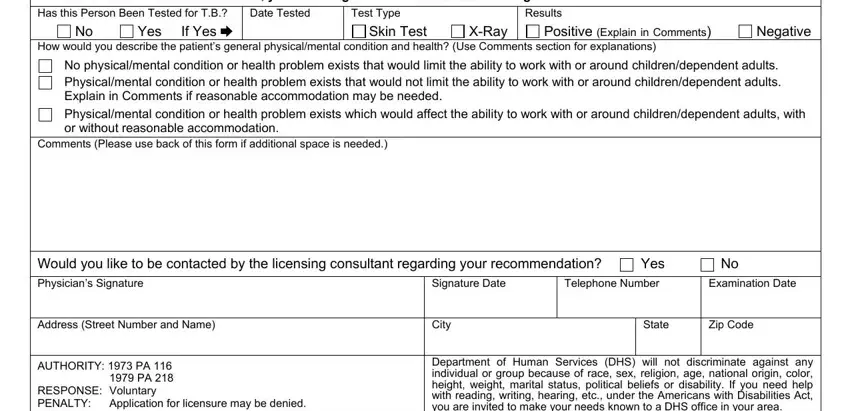
Be extremely mindful while completing XRay and Results, since this is the part in which most people make mistakes.
Step 3: Check that the information is correct and then simply click "Done" to continue further. Go for a free trial option at FormsPal and acquire immediate access to 24-Hour - accessible inside your FormsPal cabinet. FormsPal offers risk-free document editor with no personal information record-keeping or any kind of sharing. Be assured that your information is secure here!