
In case you would like to fill out michigan resident care, you don't need to download any kind of applications - just make use of our online PDF editor. Our editor is continually developing to provide the best user experience achievable, and that is because of our dedication to continual enhancement and listening closely to testimonials. All it requires is a couple of easy steps:
Step 1: Hit the orange "Get Form" button above. It'll open up our pdf tool so that you could start completing your form.
Step 2: When you access the tool, you'll see the form prepared to be filled out. Besides filling in different fields, it's also possible to do some other things with the file, namely putting on any textual content, editing the initial textual content, adding illustrations or photos, putting your signature on the PDF, and more.
This PDF will need particular data to be entered, hence be sure you take whatever time to type in what is expected:
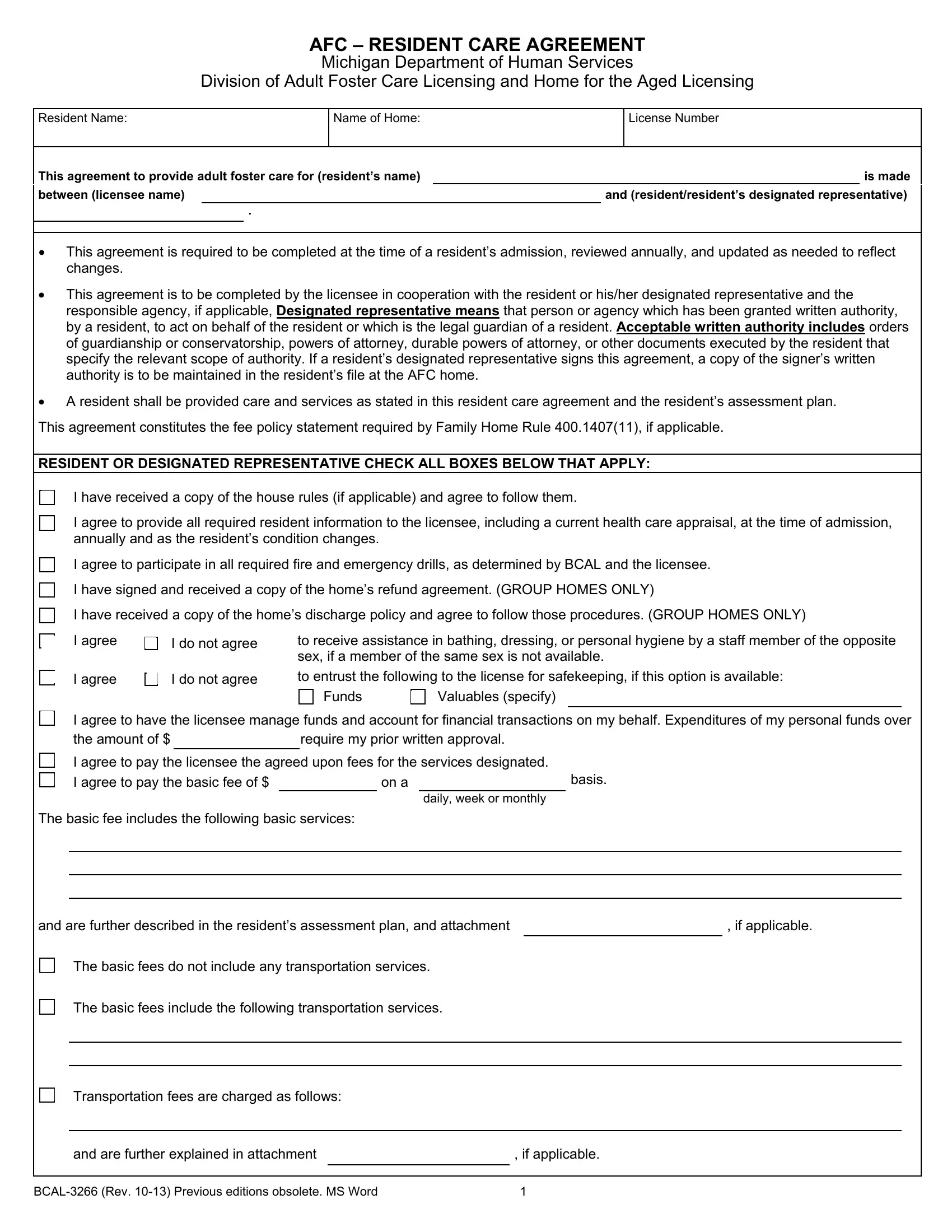
1. The michigan resident care requires specific details to be typed in. Make sure the subsequent blank fields are finalized:
2. After completing the previous part, go on to the next step and fill in all required details in these blanks - I agree to participate in all, I do not agree, to receive assistance in bathing, I agree to have the licensee, Valuables specify, Funds, I agree, I do not agree, the amount of , require my prior written approval, I agree to pay the licensee the, on a, daily week or monthly, basis, and The basic fee includes the.
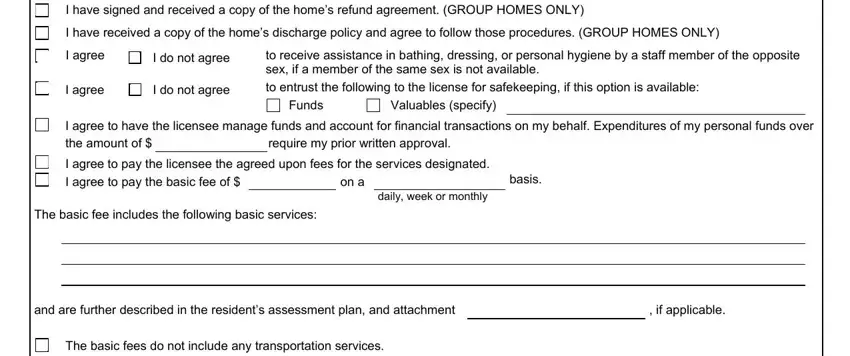
Be very mindful when completing I do not agree and I agree to participate in all, as this is the part where a lot of people make some mistakes.
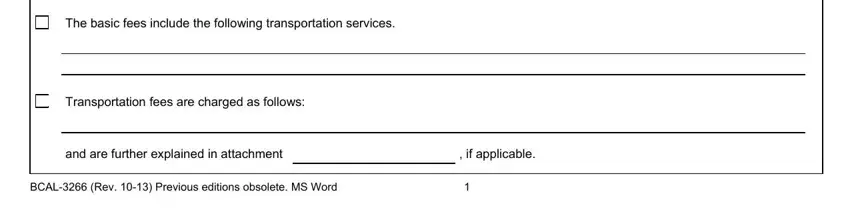
3. This next segment will be about The basic fees include the, Transportation fees are charged as, and are further explained in, if applicable, and BCAL Rev Previous editions - complete every one of these blank fields.
4. This next section requires some additional information. Ensure you complete all the necessary fields - I agree to additional services, Such additional, services may include but are not, If applicable I have read the, acknowledge that additional, BY MY SIGNATURE BELOW I AFFIRM, I have provided the resident with, I have provided the resident with, I have provided the resident with, and I agree to provide personal care - to proceed further in your process!
5. Now, this last portion is what you should complete prior to closing the document. The fields you're looking at are the following: SIGNATURES Resident, Residents Designated, LicenseeLicensee Designee, Responsible Agency if applicable, Date, Date, Date, Date, Compliments comments andor, Complaints only can also be made, PA , AUTHORITY COMPLETION Mandatory, Violation of Adult Foster Care, and Department of Human Services DHS .
Step 3: Make sure that the information is accurate and then click "Done" to complete the process. Try a free trial option with us and get immediate access to michigan resident care - downloadable, emailable, and editable in your FormsPal account page. FormsPal offers safe form completion devoid of personal information record-keeping or sharing. Rest assured that your information is in good hands here!