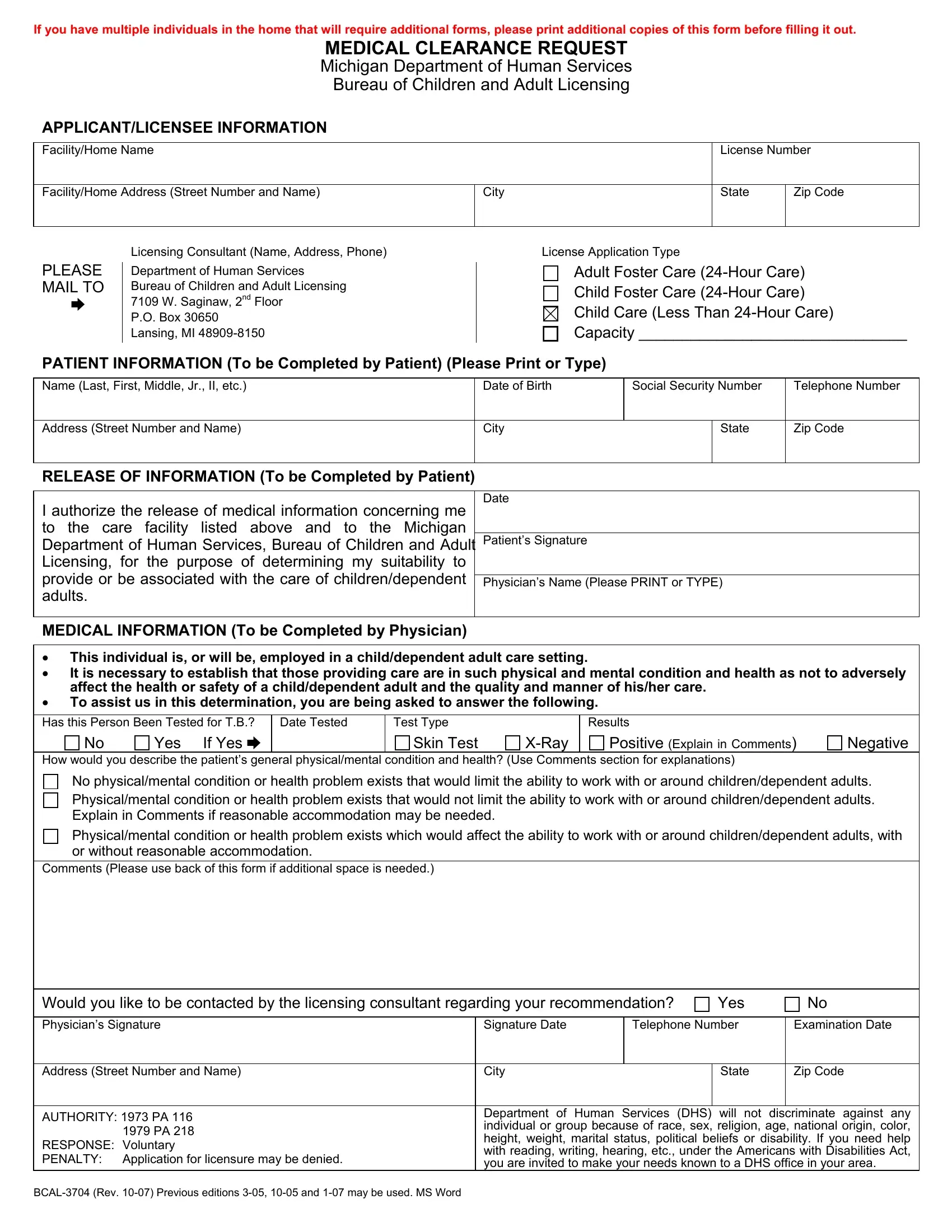
In the realm of caregiving, whether for children, adults, or dependent adults, ensuring the health and safety of those under care is paramount. The BCAL 3704 form plays a crucial role in this process, serving as a medical clearance request to the Michigan Department of Human Services, Bureau of Children and Adult Licensing. Primarily used by individuals seeking to work in facilities like adult foster care, child foster care, and child care centers, this document requires thorough information ranging from personal details of the applicant or licensee, such as their name, address, and social security number, to specific medical information provided by a physician. The form’s purpose is to establish that the individual's physical and mental health does not pose any risk to the health and safety of those they will be caring for. It covers testing for tuberculosis, general health conditions, and any potential limitations or accommodations needed. Designed to uphold stringent health standards, the completion and submission of this form are voluntary; however, failing to do so may result in the denial of a license application. The BCAL 3704 emphasizes the importance of transparency and health safety in environments where the vulnerable are cared for, reflecting the state’s commitment to protect its residents through diligent oversight.
| Question | Answer |
|---|---|
| Form Name | Bcal 3704 Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | X-Ray, DHS, Licensing, suitability |