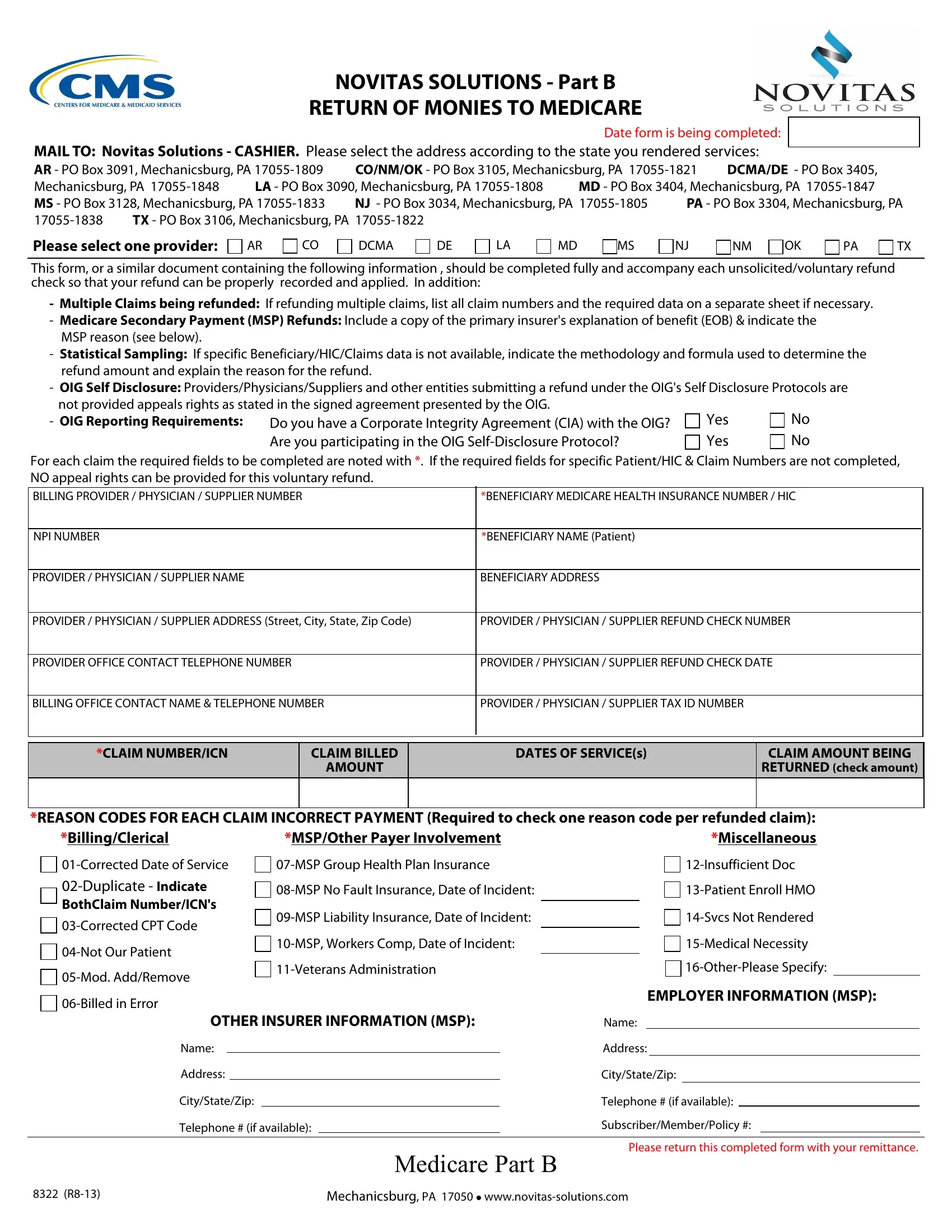
The Novitas Form 8322 is a crucial document for healthcare providers, enabling them to return funds to Medicare accurately. This procedure is essential when providers identify payments received in error or when adjustments to previously filed claims are necessary. The form is designed to be comprehensive, allowing for the recording and appropriate application of unsolicited or voluntary refunds to Medicare. It ensures that each reimbursement is accurately matched to the specific claim it addresses by requiring detailed information for each refunded claim, including provider identifiers, beneficiary details, and claim data. Providers can use the form to list multiple claims, include Medicare Secondary Payment (MSP) refunds with necessary supporting documents, and specify the reasons for the refunds using designated codes. Noteworthy, for those under OIG scrutiny or adhering to a Corporate Integrity Agreement, the form also addresses specific protocols for submitting refunds without conceding appeal rights. The Novitas Solutions addresses vary by the state in which the services were rendered, highlighting the tailored approach to processing refunds efficiently and securely. This form represents a significant aspect of maintaining compliance and transparency in healthcare billing practices, ensuring that Medicare funds are utilized correctly and responsibly.
| Question | Answer |
|---|---|
| Form Name | Novitas Form 8322 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | insurer, MSP, TX, NM |