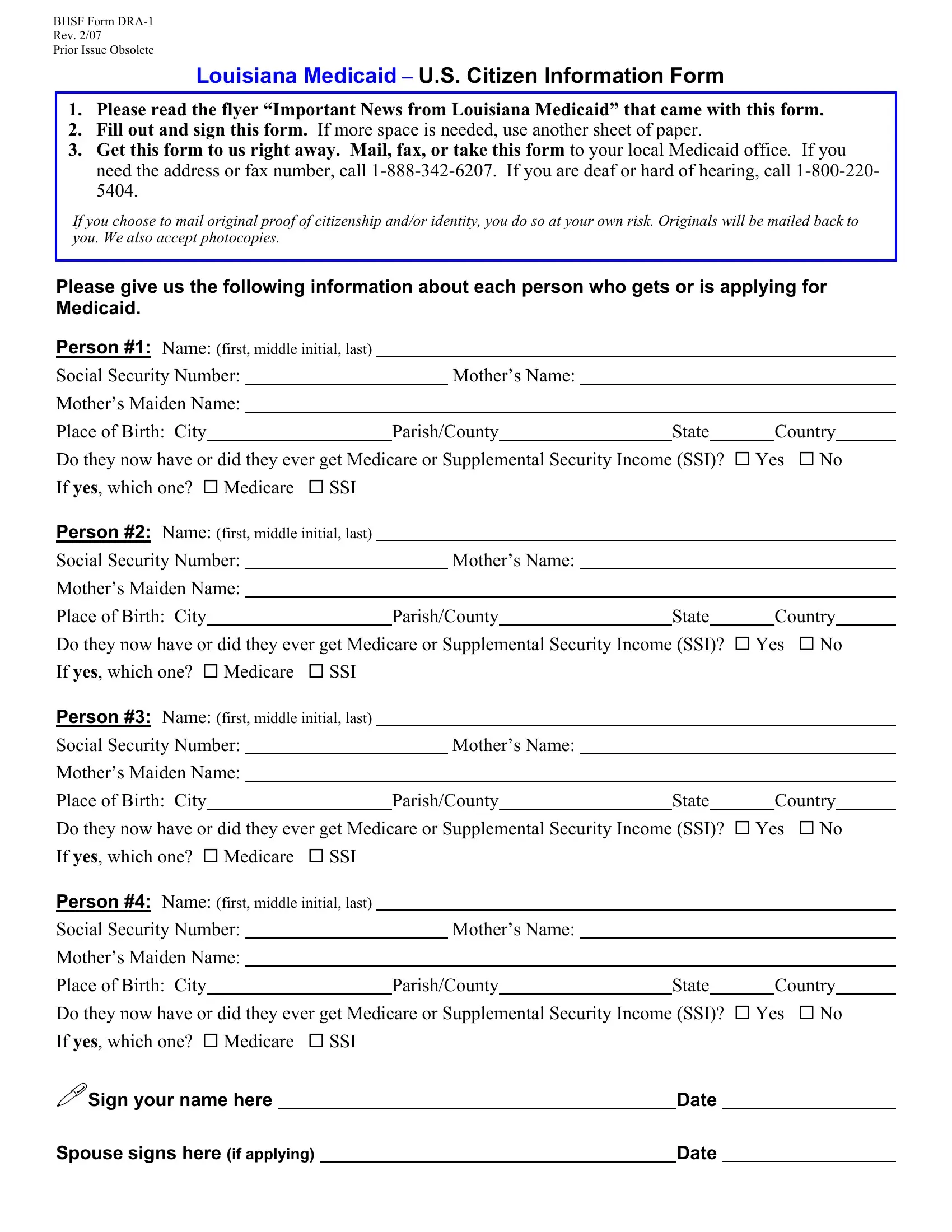
The BHSF Form DRA-1, a crucial document for Louisiana Medicaid applicants, serves a vital purpose in verifying U.S. citizenship for individuals seeking Medicaid benefits. Updated in February 2007, this form requires applicants to provide comprehensive personal information, including name, social security number, mother's name and maiden name, and place of birth. Furthermore, it inquires about whether the applicant has received or is currently receiving Medicare or Supplemental Security Income (SSI). The form comes with instructions emphasizing the importance of reading the accompanying "Important News from Louisiana Medicaid" flyer, filling out the form thoroughly, and promptly submitting it through mail, fax, or in person to a local Medicaid office. Contact information for assistance is provided, including phone numbers for general inquiries and a dedicated line for individuals who are deaf or hard of hearing. Applicants are cautioned that mailing original documents of proof of citizenship and identity carries a risk, though originals will be returned, and photocopies are acceptable. This form reflects the administrative procedures put in place to ensure that Medicaid applicants are indeed U.S. citizens, an essential step in the eligibility verification process for receiving healthcare benefits under the Medicaid program.
| Question | Answer |
|---|---|
| Form Name | Bhsf Form Dra 1 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | photocopies, Supplemental, Spouse, Obsolete |
BHSF Form
Rev. 2/07
Prior Issue Obsolete
Louisiana Medicaid – U.S. Citizen Information Form
1.Please read the flyer “Important News from Louisiana Medicaid” that came with this form.
2.Fill out and sign this form. If more space is needed, use another sheet of paper.
3.Get this form to us right away. Mail, fax, or take this form to your local Medicaid office. If you need the address or fax number, call
If you choose to mail original proof of citizenship and/or identity, you do so at your own risk. Originals will be mailed back to you. We also accept photocopies.
Please give us the following information about each person who gets or is applying for Medicaid.
Person #1: Name: (first, middle initial, last) |
|
|
|
|
|
|
|
|
|
|||||||||
Social Security Number: |
|
|
|
|
Mother’s Name: |
|
|
|
|
|
|
|
|
|
||||
Mother’s Maiden Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Place of Birth: City |
|
|
|
|
|
|
Parish/County |
|
|
State |
|
|
Country |
|
||||
Do they now have or did they ever get Medicare or Supplemental Security Income (SSI)? |
Yes |
No |
||||||||||||||||
If yes, which one? |
Medicare |
SSI |
|
|
|
|
|
|
|
|
|
|||||||
Person #2: Name: (first, middle initial, last) |
|
|
|
|
|
|
|
|
|
|||||||||
Social Security Number: |
|
|
|
|
Mother’s Name: |
|
|
|
|
|
|
|
|
|
||||
Mother’s Maiden Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Place of Birth: City |
|
|
|
|
|
|
Parish/County |
|
|
State |
|
|
Country |
|
||||
Do they now have or did they ever get Medicare or Supplemental Security Income (SSI)? |
Yes |
No |
||||||||||||||||
If yes, which one? |
Medicare |
SSI |
|
|
|
|
|
|
|
|
|
|||||||
Person #3: Name: (first, middle initial, last) |
|
|
|
|
|
|
|
|
|
|||||||||
Social Security Number: |
|
|
|
|
Mother’s Name: |
|
|
|
|
|
|
|
|
|
||||
Mother’s Maiden Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Place of Birth: City |
|
|
|
|
|
|
Parish/County |
|
|
State |
|
|
Country |
|
||||
Do they now have or did they ever get Medicare or Supplemental Security Income (SSI)? |
Yes |
No |
||||||||||||||||
If yes, which one? |
Medicare |
SSI |
|
|
|
|
|
|
|
|
|
|||||||
Person #4: Name: (first, middle initial, last) |
|
|
|
|
|
|
|
|
|
|||||||||
Social Security Number: |
|
|
|
|
Mother’s Name: |
|
|
|
|
|
|
|
|
|
||||
Mother’s Maiden Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Place of Birth: City |
|
|
|
|
|
|
Parish/County |
|
|
State |
|
|
Country |
|
||||
Do they now have or did they ever get Medicare or Supplemental Security Income (SSI)? |
Yes |
No |
||||||||||||||||
If yes, which one? |
Medicare |
SSI |
|
|
|
|
|
|
|
|
|
|||||||
Sign your name here |
|
|
|
|
|
|
|
|
Date |
|
|
|
|
|
||||
Spouse signs here (if applying) |
|
Date |