
How to Fill Out the BHSF Newborn Request Form
Follow these steps to complete the form correctly and avoid processing delays:
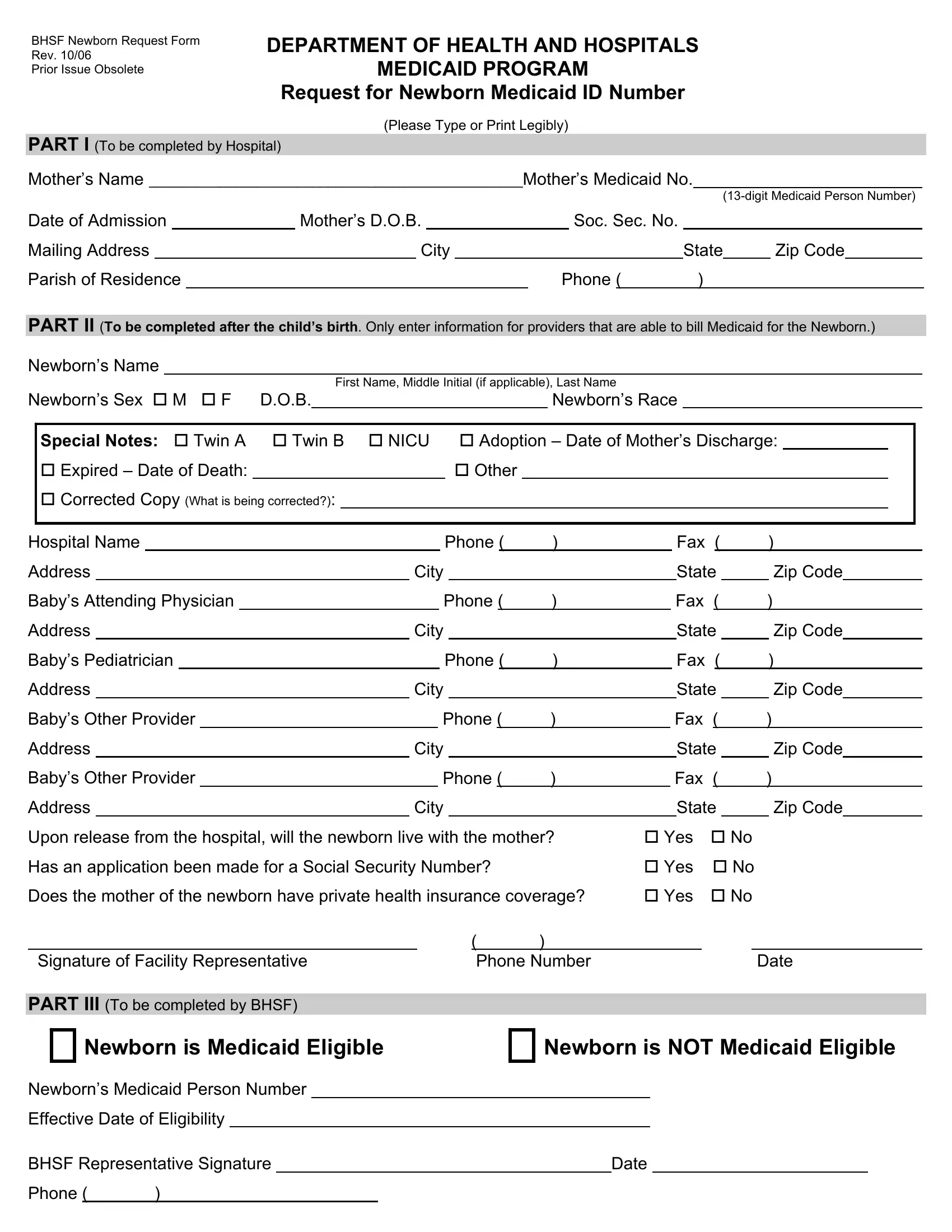
- Download the current version. Use the PDF available on FormsPal. Only the October 2006 revision is accepted by BHSF. Earlier versions are obsolete.
- Complete Part I before delivery. Hospital staff fill in the mother's full name, Medicaid number, date of birth, and contact details.
- Complete Part II after the baby is born. Enter the newborn's date of birth, sex, weight, and the name of the healthcare provider billing Medicaid. Note any special circumstances such as twin births or adoption.
- Answer the discharge questions. The form asks where the baby will live after leaving the hospital and whether a Social Security number application has been filed.
- Submit the completed form to BHSF. BHSF representatives complete Part III and confirm the newborn's Medicaid eligibility. Keep a copy for your records.
What Common Mistakes Should You Avoid?
The most common errors are missing fields and illegible handwriting. Always double-check the mother's Medicaid number. For twins or multiple births, a separate BHSF Newborn Request Form may be required for each child.
You may also need these related forms: