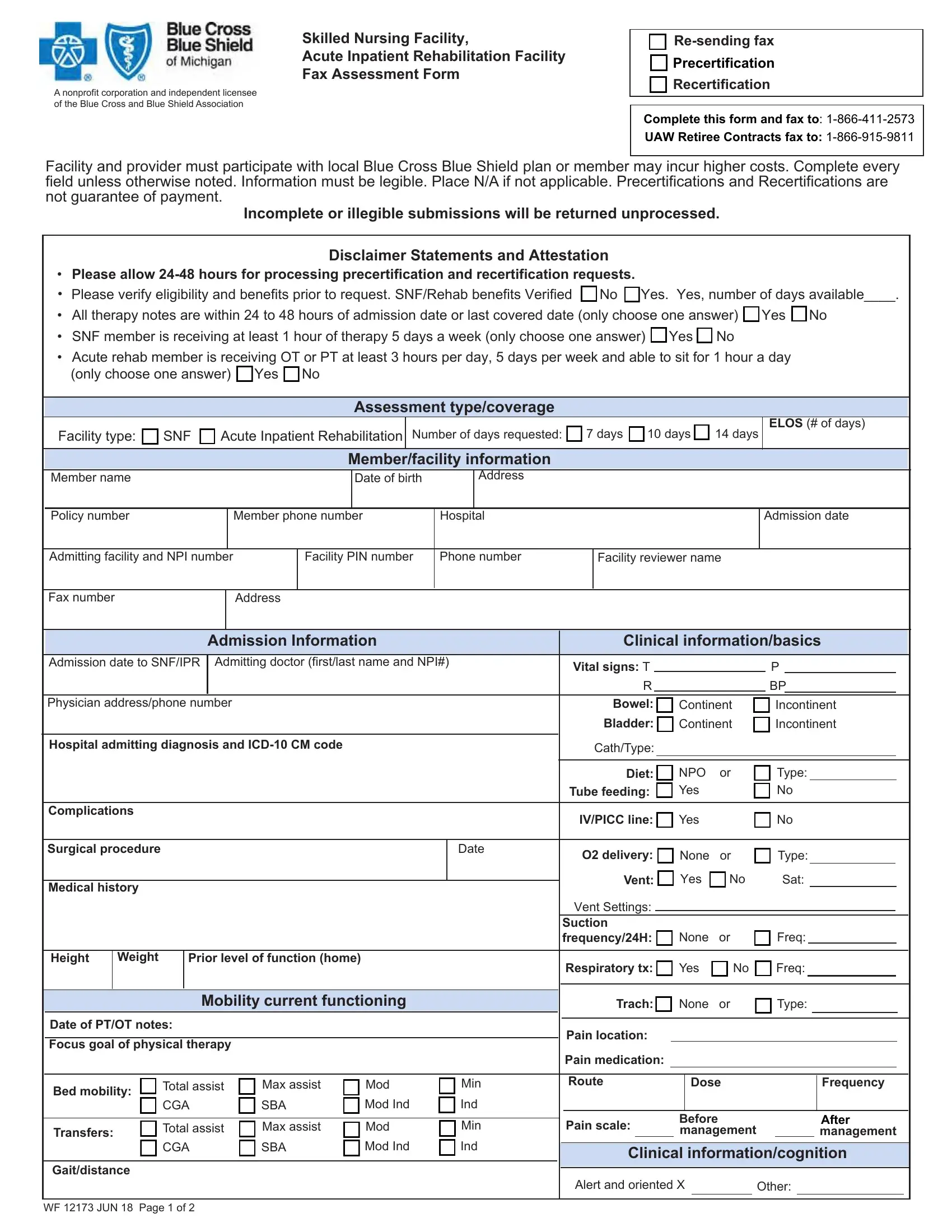
The intricate process of transitioning a patient from hospital care back to their home or another facility is encapsulated within the Hospital Patient Discharge form, showcasing a comprehensive range of assessments and necessary information to ensure a smooth transition. This form, utilized by skilled nursing facilities and acute inpatient rehabilitation facilities, serves as a critical tool for communicating the patient's care needs and planning post-hospital care. It encompasses a variety of sections including facility and member information, detailed clinical information from admission details to medical history, therapy requirements, and discharge plans. Precertification and recertification processes are integral to this paperwork, emphasizing the need for accuracy and thoroughness in completion to avoid delays in processing. Importantly, this form underscores the partnership with Blue Cross and Blue Shield Association, highlighting the necessity for facilities and providers to participate with the local plan to mitigate potential increased costs for members. Key to this form are disclaimers and attestations regarding the processing time for requests, the verification of eligibility and benefits, and a clear statement that the completion of this document does not guarantee payment. This emphasizes the meticulous attention required in filling out the form, where every field demands attention, and any oversight or illegibility could lead to unprocessed submissions. Furthermore, the form incorporates significant medical details—ranging from admitting diagnosis and vital signs to a comprehensive review of the patient’s functional status and planned discharge details—ensuring a holistic view of the patient's needs and facilitating a seamless transition from hospital to the next phase of care.
| Question | Answer |
|---|---|
| Form Name | Hospital Patient Discharge Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | michigan facility form, michigan acute inpatient facility, skilled nursing form, printable discharge patient registration forms |