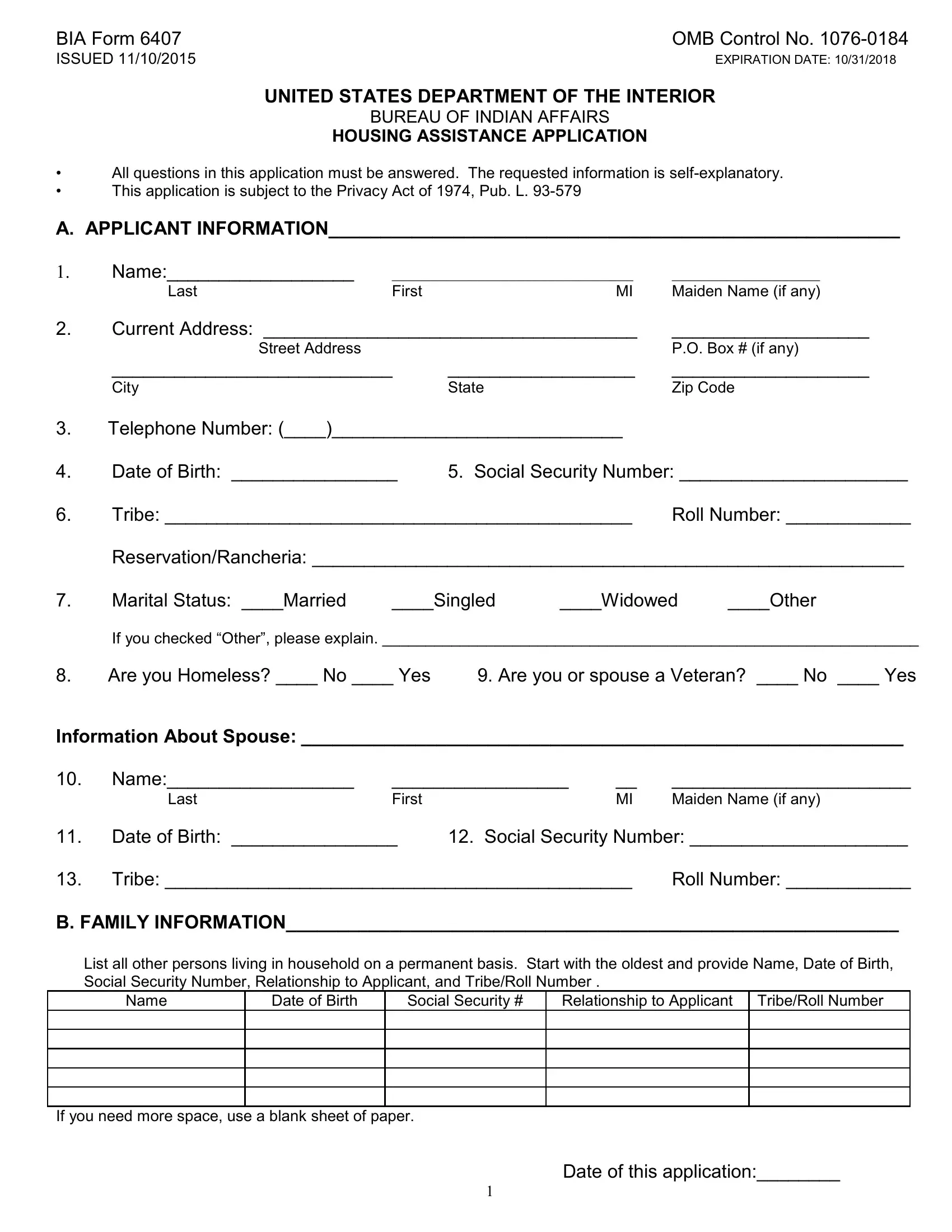
In a landscape where the intricate layers of policy, privacy, and eligibility converge, the BIA Form 6407 emerges as a vital document for those seeking housing assistance within indigenous communities. Issued by the United States Department of the Interior, Bureau of Indian Affairs, on November 10, 2015, with an expiration date of October 31, 2018, this form embodies the governmental response to the housing needs of Native American families. It meticulously outlines the procedure and requirements for applying for housing assistance, emphasizing the need for complete and accurate information across several domains: applicant information, family composition, income details, housing conditions, land ownership, and general personal circumstances. Designed under the scaffolding of the Privacy Act of 1974, the form serves not just as an application but also as a guardian of applicants' sensitive data, ensuring that such information is handled with utmost confidentiality and integrity. Moreover, it mandates the disclosure of a broad spectrum of data, from the biographical (name, age, marital status) and financial (income sources, total household income) to specifics about the housing needs (repair, renovation, or construction) and the status of the land where such housing activities are proposed. This thorough collection of data underscores the form's role in weaving a detailed narrative of each applicant’s situation, thereby facilitating a fair and comprehensive evaluation process for housing assistance eligibility under the Housing Improvement Program.
| Question | Answer |
|---|---|
| Form Name | Bia Form 6407 |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | form 6407 form, at t 6407 form, bia form 6407, bia unhcr form |
BIA Form 6407 |
OMB Control No. |
ISSUED 11/10/2015 |
EXPIRATION DATE: 10/31/2018 |
|
UNITED STATES DEPARTMENT OF THE INTERIOR |
|
BUREAU OF INDIAN AFFAIRS |
|
HOUSING ASSISTANCE APPLICATION |
•All questions in this application must be answered. The requested information is
•This application is subject to the Privacy Act of 1974, Pub. L.
A. APPLICANT INFORMATION_______________________________________________________
1. |
Name:__________________ |
_______________________________ |
___________________ |
|
|
Last |
First |
MI |
Maiden Name (if any) |
2. |
Current Address: ____________________________________ |
___________________ |
||
|
Street Address |
|
|
P.O. Box # (if any) |
|
___________________________ |
__________________ |
___________________ |
|
|
City |
|
State |
Zip Code |
3.Telephone Number: (____)____________________________
4. |
Date of Birth: ________________ |
5. Social Security Number: ______________________ |
||||
6. |
Tribe: _____________________________________________ |
Roll Number: ____________ |
||||
|
Reservation/Rancheria: _________________________________________________________ |
|||||
7. |
Marital Status: ____Married |
____Singled |
____Widowed |
____Other |
||
|
If you checked “Other”, please explain. ______________________________________________________________ |
|||||
8. |
Are you Homeless? ____ No ____ Yes |
9. Are you or spouse a Veteran? ____ No ____ Yes |
||||
Information About Spouse: __________________________________________________________
10. |
Name:__________________ |
_________________ |
__ |
_______________________ |
|
|
Last |
First |
|
MI |
Maiden Name (if any) |
11. |
Date of Birth: ________________ |
12. Social Security Number: _____________________ |
|||
13. |
Tribe: _____________________________________________ |
Roll Number: ____________ |
|||
B. FAMILY INFORMATION___________________________________________________________
List all other persons living in household on a permanent basis. Start with the oldest and provide Name, Date of Birth, Social Security Number, Relationship to Applicant, and Tribe/Roll Number .
Name |
Date of Birth |
Social Security # |
Relationship to Applicant |
Tribe/Roll Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
If you need more space, use a blank sheet of paper.
Date of this application:________
1
BIA Form 6407 |
OMB Control No. |
ISSUED 11/10/2015 |
EXPIRATION DATE: 10/31/2018 |
C. INCOME INFORMATION_________________________________________________________
14. Earned Income: Start with applicant, then list all permanent family members, including all who are listed under Parts A and B and have earned income. Provide signed copy of
Name
Annual Earned Income
Source of Income
Total annual earned income: $ ____________________________
15. Unearned Income: Start with applicant, then list all permanent family members, including all who are listed under Parts A and B and have unearned income such as social security, retirement, disability and unemployment benefits, child support and alimony, royalties, per capita payments, interest, etc. Provide check stubs, statements, individual Indian Money (IIM) ledgers, etc. for verification.
Name
Annual Unearned Income
Source of Income
Total annual unearned income: $ ____________________________
16. TOTAL COMBINED ANNUAL HOUSEHOLD INCOME (earned + unearned): $ ___________________
D. HOUSING INFORMATION________________________________________________________
17.Location of the house to be repaired, renovated or constructed. (Give address and detailed directions to this house). **DRAW MAP ON BACK OF THIS PAGE**
18.Provide a brief description of the problems you are experiencing with your house or the type of housing assistance for which you are applying.
19.If repair assistance is needed, do you own _____ or rent _____ this house?
If renting, is the owner Indian? ____No ____ Yes
If yes, provide name of owner(s):
20.Are you living in Overcrowded Conditions? ____ No ____ Yes
21.Is the condition of the home in a dilapidated state? ____ No ____ Yes
Date of this application:________
2
BIA Form 6407 |
OMB Control No. |
ISSUED 11/10/2015 |
EXPIRATION DATE: 10/31/2018 |
HOUSING INFORMATION, continued. |
|
22.
23.
Is electricity available? |
____No ____Yes |
If yes, provide name of electric company: _______________. |
||||||
Type of Sewer system: |
|
___ City Sewer |
|
___ Septic Tank |
|
___ Chemical Toilet |
|
___ Outhouse |
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
Water Source: ____ City Water |
____ Private Well |
____ Community Water Tank |
|
||||
|
____ Other (Please describe): |
|
|
|
|
|
|
|
24. |
No. of Bedrooms ____. |
|
|
|
|
|
|
|
25. |
House Size: _____ (Square Feet) |
|
[ LENGTH _____ ft/in] |
[WIDTH _____ |
ft/in] |
|||
26. |
Bathroom facilities in existing house: |
|
|
|
Facility |
Yes |
|
No |
|
|
|
Flush toilet |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
Bathtub |
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
Sink/lavatory |
|
|
|
||
|
|
|
|
|
|
|
|
|
E. LAND INFORMATION____________________________________________________________
27. |
Do you own the land on which you wish to renovate or build this home? _____ Yes |
_____ No |
|||||
|
If no, can you provide proof that you can obtain land? ____ Yes |
_____ No |
|
|
|||
|
Provide the name of the owner(s): |
|
|
|
|
|
|
28. |
What is the current |
___ Fee |
___ Tribal Fee |
|
|
___ Native/Restricted |
|
|
status of the land? |
___ Individual trust land |
___ Tribal trust land |
|
|
___ Public Domain |
|
|
|
___ Individually restricted |
___ Tribally restricted |
|
___ Other: |
||
|
|
|
|
|
|
|
|
29.
If you do not own the land, do you have: _____ Leasehold interest? ____ Use permit?
______ Indefinite assignment or joint ownership? If so, please explain:
F. GENERAL INFORMATION________________________________________________________
|
|
|
|
Yes |
|
No |
30. |
Have you or anyone in your household ever received Housing Improvement |
|
|
|
||
|
Program assistance? |
|
|
|
|
|
|
If yes, give amount received $_______; the year it was received: 19__ __; and the location |
|
|
|
||
|
of the house: |
|
|
|
|
|
31. |
Do you own any other house not occupied by your family? |
|
|
|
||
|
If yes, state where the house is located: ____________ and who occupies it: __________. |
|
|
|
||
|
|
|
|
|
||
32. |
Do you live in a house built with Housing and Urban Development (HUD) funds? |
|
|
|
||
33. |
Is the HUD project still under operation of an Indian Housing Authority? |
|
|
|
||
34. |
Are you seeking Down Payment Assistance? |
|
|
|
||
|
If yes, have you applied with USDA Rural Development or other lending institution? Please |
|
|
|
||
|
provide a copy of the credit letter. |
|
|
|
|
|
35. |
If you are requesting assistance for a new housing unit, have you applied for |
|
|
|
||
|
assistance from: |
|
|
|
|
|
|
• |
Indian Housing Authority? |
If yes, provide date of application:____________ |
|
|
|
|
• |
Tribal Credit Program? |
If yes, provide date of application:____________ |
|
|
|
|
• |
Other? From who:___________ |
If yes, provide date of application:____________ |
|
|
|
36. |
Does anyone in your family, who is a permanent resident listed under Parts A and B |
|
|
|
||
|
of this application, have a severe health problem, handicap or permanent disability? |
|
|
|
||
|
|
|
|
|||
|
If yes, provide name of family member __________________ and brief description of condition. (Your servicing |
|||||
|
housing office will advise you if you must provide a statement of condition from one source, which may include a |
|||||
|
physician’s certification, Social Security or Veterans Affairs determination, or similar determination). |
|
||||
|
|
|
Date of this application:________ |
|
||
|
|
|
3 |
|
|
|
BIA Form 6407 |
OMB Control No. |
ISSUED 11/10/2015 |
EXPIRATION DATE: 10/31/2018 |
G.APPLICANT CERTIFICATION ____________________________________________________
(Read this certification carefully before you sign and date your application. Sign in ink).
I certify that all the answers given are true, complete and correct to the best of my knowledge and belief, and they are made in good faith. This certification is made with the knowledge that the information will be used to determine eligibility to receive financial assistance, and that false or misleading statements may constitute a violation of 18 U.S.C. 1001.
This application contains material covered by the Privacy Act. No record will be communicated to anyone or any agency unless requested in writing, by the applicant, or unless an officer or employee of the housing program or other Federal agency requires it in the performance of their duties.
Applicant’s Signature: ___________________________________ |
Date: |
______________ |
Spouse’s Signature (if appropriate) _________________________ |
Date: |
______________ |
PRIVACY ACT STATEMENT
25 CFR 265 and 25 U.S.C. 13 authorize the collection of this information. This information is covered by the system of record notice “Indian Housing Improvement Program, Interior,
PAPERWORK REDUCTION ACT STATEMENT
This information is being collected to select eligible families or individuals to participate in the Housing Improvement Program. Response to this request is required to obtain a benefit in accordance with 25 CFR 256. You are not required to respond to this collection of information unless it displays a currently valid OMB control number. This information will be used to determine the eligibility and the ranking of the applicant. Public reporting burden for this form is estimated to average 1 hour per response, including the time for reviewing instructions, gathering and maintaining data, and completing and reviewing the form. Direct comments regarding the burden estimate or any other aspect of this form to Information Collection Clearance Officer – Indian Affairs, 1849 C Street, NW,
Date of this application:________
4