In an era where health and wellness are increasingly prioritized, the BMC HealthNet Plan offers a unique opportunity for its members to maintain a healthy lifestyle through financial support for fitness expenses. With the MassHealth Fitness Reimbursement Form, individuals who have been members of both a health or fitness club and the BMC HealthNet Plan’s MassHealth plan simultaneously for at least three months in a calendar year can seek reimbursement. This initiative underscores the importance of encouraging physical activity among community members by offering up to $200 per family each year to cover fitness-related costs. It's essential that the form, along with necessary documentation such as receipts and a copy of the Health Club Agreement, is submitted no later than March 31 of the following year to be eligible for this benefit. This detailed process not only showcases BMC HealthNet Plan’s commitment to supporting its members' health and wellness journey but also emphasizes the plan's structured approach to ensuring members maximize their entitled benefits efficiently and effectively. The incorporation of member information and certification sections within the form also illustrates an organized method to authenticate and process requests, thereby fostering transparency and trust between the healthcare provider and its members.
| Question | Answer |
|---|---|
| Form Name | Bmc Healthnet Plan Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | HealthNet, certify, MassHealth, bmc health net viscosupplemental form pdf |
bmchp.org |
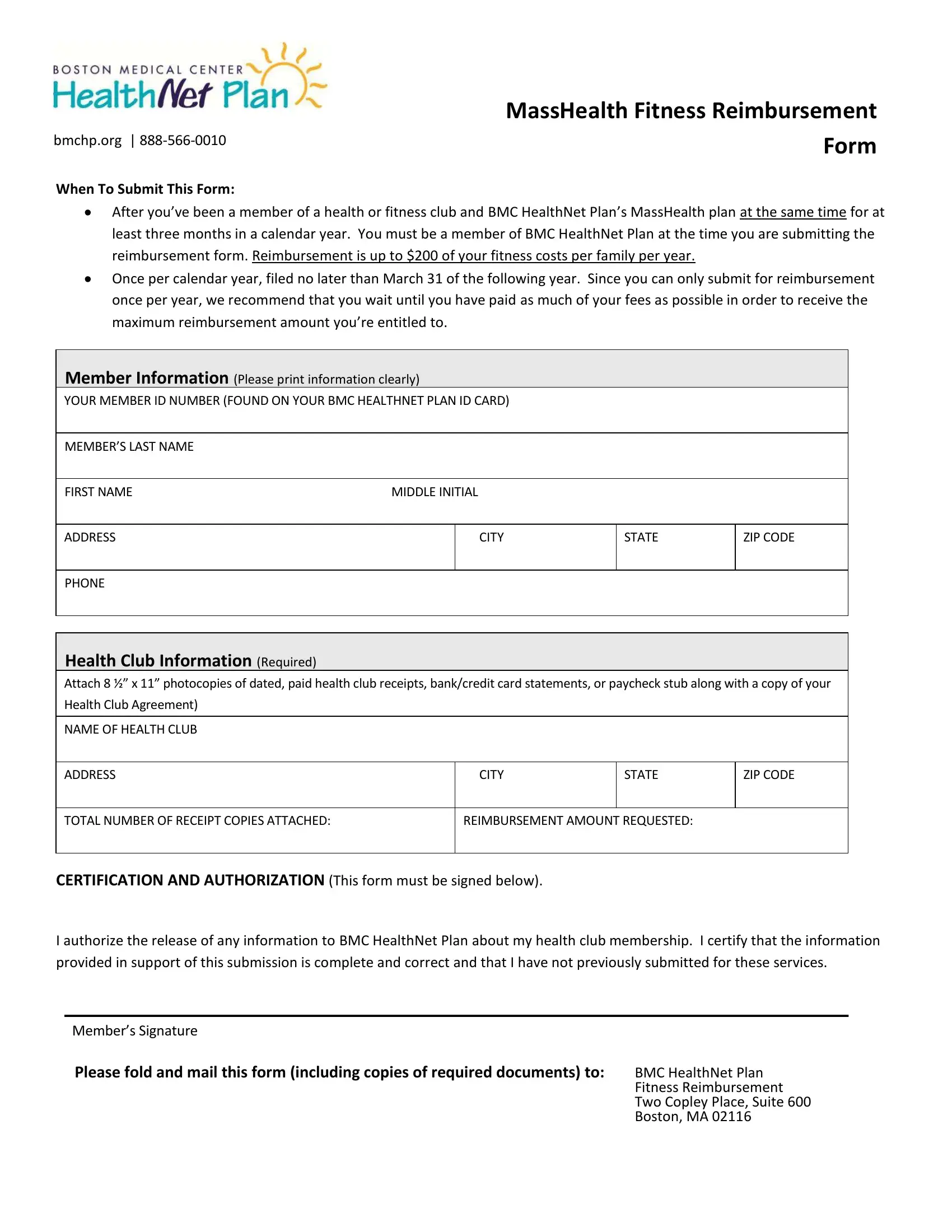
When To Submit This Form:
MassHealth Fitness Reimbursement
Form
After ou’ e ee a e er of a health or fit ess lu a d BMC HealthNet Plan’s MassHealth pla at the same time for at
least three months in a calendar year. You must be a member of BMC HealthNet Plan at the time you are submitting the reimbursement form. Reimbursement is up to $200 of your fitness costs per family per year.
Once per calendar year, filed no later than March 31 of the following year. Since you can only submit for reimbursement once per year, we recommend that you wait until you have paid as much of your fees as possible in order to receive the
a i u rei urse e t a ou t ou’re e titled to.
Member Information (Please print information clearly)
YOUR MEMBER ID NUMBER (FOUND ON YOUR BMC HEALTHNET PLAN ID CARD)
MEMBER’S LAST NAME
FIRST NAME |
MIDDLE INITIAL |
ADDRESS
CITY
STATE
ZIP CODE
PHONE
Health Club Information (Required)
Attach 8 ½” 11” photo opies of dated, paid health lu re eipts, a k/ redit ard state e ts, or pa he k stu alo g ith a op of your Health Club Agreement)
NAME OF HEALTH CLUB
ADDRESS
CITY
STATE
ZIP CODE
TOTAL NUMBER OF RECEIPT COPIES ATTACHED:
REIMBURSEMENT AMOUNT REQUESTED:
CERTIFICATION AND AUTHORIZATION (This form must be signed below).
I authorize the release of any information to BMC HealthNet Plan about my health club membership. I certify that the information provided in support of this submission is complete and correct and that I have not previously submitted for these services.
Me er’s Sig ature
Please fold and mail this form (including copies of required documents) to: |
BMC HealthNet Plan |
|
Fitness Reimbursement |
|
Two Copley Place, Suite 600 |
|
Boston, MA 02116 |