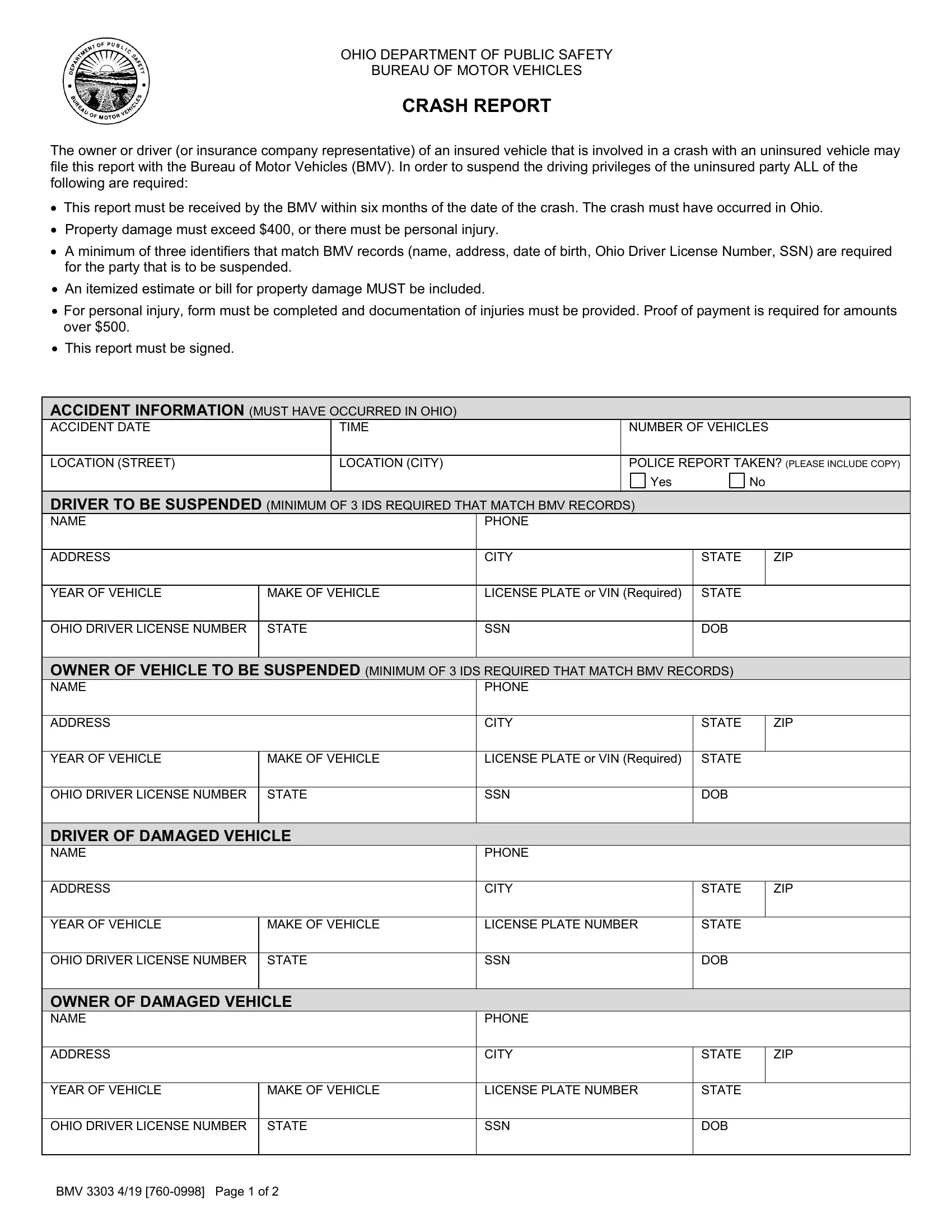

The Ohio BMV 3303 form is a two-page document that you can complete and submit online through our PDF editor. This report is required when an insured vehicle is involved in a crash with an uninsured driver in Ohio. Below is a step-by-step overview of each section to help you fill it out correctly.
Step 1: Click the "Get Form" button above to open the document in our online editor. Begin with the top section, which asks for your personal details and the date and location of the crash. You will need to provide your full name, address, phone number, date of birth, and Social Security number.
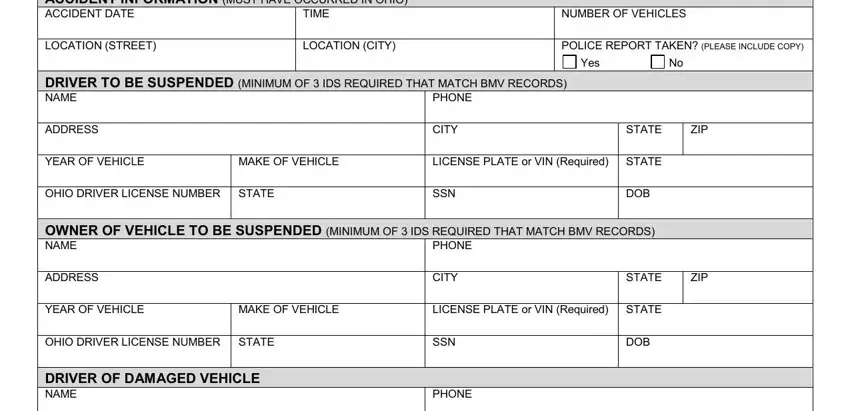
Step 2: Enter information about the vehicles involved in the accident. For each vehicle, you will need the driver's name, the vehicle owner's name, the make and model of the vehicle, the state of registration, the license plate number, and the Social Security number of the driver. Make sure to include information for both the insured and uninsured vehicles.
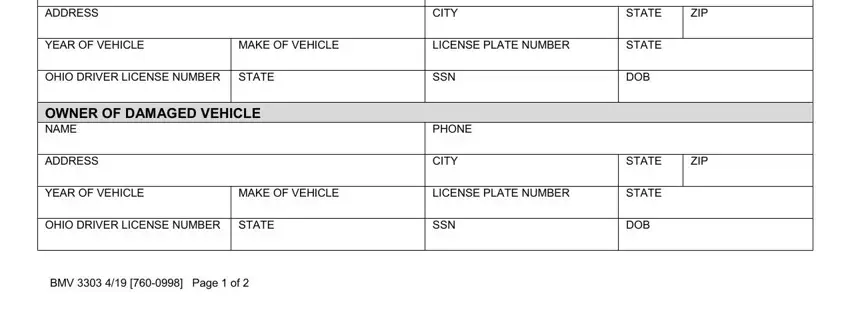
Double-check all vehicle details before moving on. The Ohio Bureau of Motor Vehicles requires at least three identifiers for the uninsured individual that match their records. Errors or missing data in this section can delay processing or result in the report being returned.
Step 3: Complete the denial of coverage section, claim information, and damage details. If the insurance company has denied coverage for the uninsured party, indicate this clearly and provide the claim number and file number. For property damage, attach an itemized estimate or repair bill showing that damages exceed the 00 minimum threshold. For personal injuries, include proof of payment for medical costs over 00.
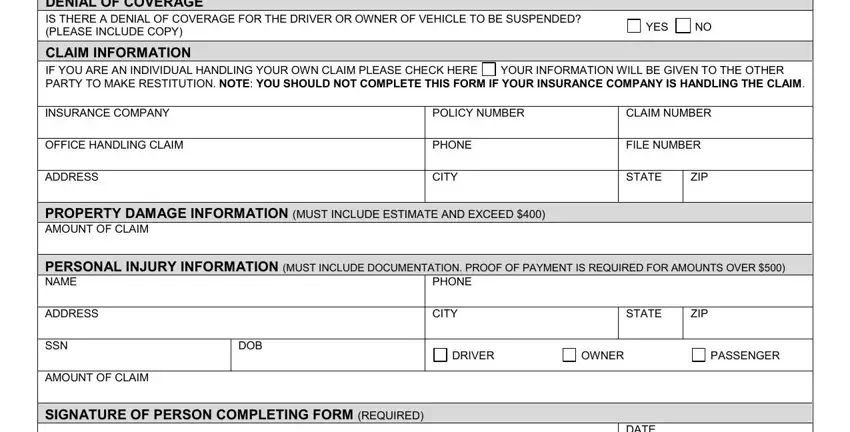
Step 4: Sign the form and review all entries for accuracy. Your signature confirms that the information is true and that your vehicle was insured at the time of the accident. Mail the completed report to the Ohio Bureau of Motor Vehicles, Compliance Unit, PO Box 16784, Columbus, OH 43216. Allow 15 business days for processing.
Frequently Asked Questions
What is the deadline for filing?
You must submit this form within six months of the accident date. Reports received after this deadline will not be processed by the Ohio Bureau of Motor Vehicles.
Who can file this report?
The insured vehicle owner, driver, or a representative of the insurance company involved in the claim can submit the report.
What happens after the form is submitted?
The Ohio Bureau of Motor Vehicles reviews the report. If the documentation is complete and the criteria are met, the driving privileges of the uninsured party may be suspended until they provide proof of financial responsibility.
What is the minimum property damage amount required?
The crash must have caused property damage exceeding 00 or resulted in a personal injury. If the damage is below this threshold and no injuries occurred, the report will not be processed.
What identifiers are needed for the uninsured driver?
You must provide at least three pieces of identifying information for the uninsured party. Acceptable identifiers include their full name, date of birth, Social Security number, driver license number, and residential address. These must match the records held by the Ohio Bureau of Motor Vehicles.
What if I need other Ohio motor vehicle forms?
FormsPal offers many Ohio government forms. You may also need the Ohio form 1173 for title transfers or the motor vehicle no-fault insurance form for insurance verification.