
With the online PDF editor by FormsPal, you're able to complete or change nf5 form fillable right here. To have our tool on the forefront of practicality, we work to integrate user-driven features and enhancements regularly. We are at all times glad to receive suggestions - help us with revampimg PDF editing. To get the ball rolling, take these simple steps:
Step 1: Access the PDF inside our editor by hitting the "Get Form Button" in the top area of this page.
Step 2: As you open the file editor, you will find the form all set to be filled out. Apart from filling out different blanks, it's also possible to perform many other things with the Document, specifically writing any text, editing the initial textual content, inserting illustrations or photos, signing the form, and a lot more.
It is straightforward to complete the document with this detailed guide! Here's what you want to do:
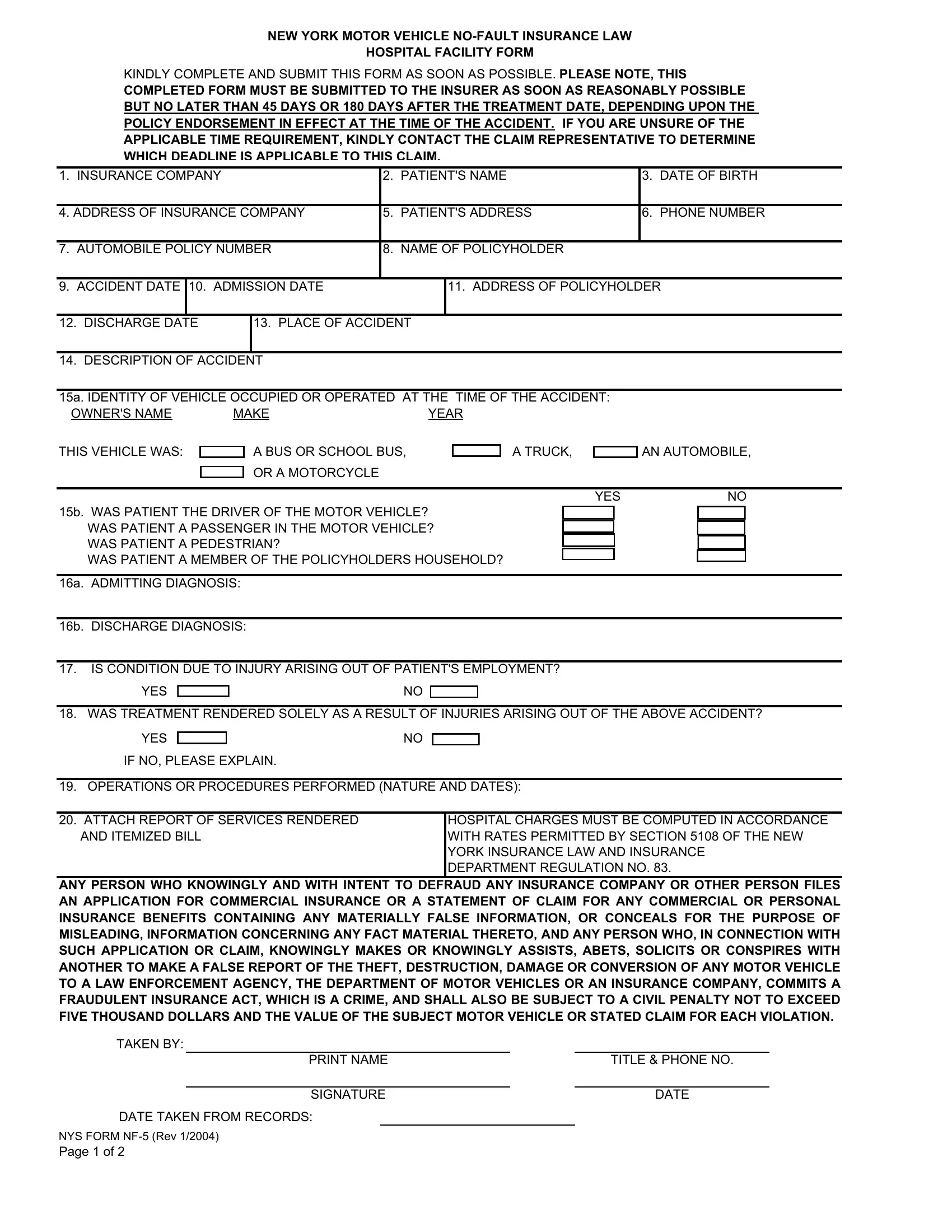
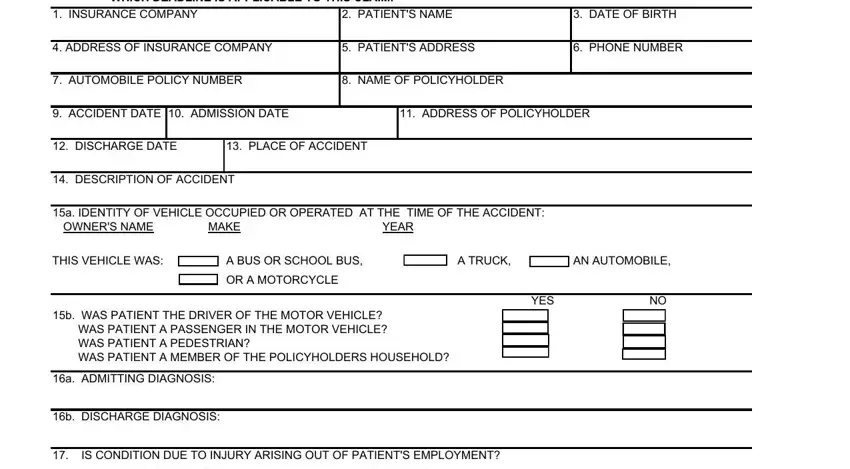
1. It is very important fill out the nf5 form fillable properly, hence be attentive while filling out the sections comprising these fields:
2. After the last section is done, you're ready insert the necessary specifics in YES, WAS TREATMENT RENDERED SOLELY AS, YES, IF NO PLEASE EXPLAIN, OPERATIONS OR PROCEDURES, ATTACH REPORT OF SERVICES, HOSPITAL CHARGES MUST BE COMPUTED, ANY PERSON WHO KNOWINGLY AND WITH, TAKEN BY, PRINT NAME, SIGNATURE, TITLE PHONE NO, DATE, DATE TAKEN FROM RECORDS, and NYS FORM NF Rev Page of in order to move forward to the next part.
3. Your next step is generally simple - fill out all of the empty fields in THE APPLICANT AUTHORIZES THE, SIGNATURE OF PATIENT PARENT OR, DATE, PATIENT Your health provider may, IF YOU HAVE CHOSEN TO AUTHORIZE, SIGNED, SIGNED, SIGNATURE OF PATIENT PARENT OR, SIGNATURE OF HOSPITAL, DATE, PATIENT Your health provider may, B YOU MAY NOT ALSO ENTER INTO AN, IF YOU HAVE CHOSEN TO ASSIGN YOUR, and ASSIGNMENT OF NOFAULT BENEFITS I in order to complete the current step.
4. The fourth paragraph comes next with these blank fields to consider: ASSIGNMENT OF NOFAULT BENEFITS I, SIGNED, SIGNATURE OF PATIENT PARENT OR, DATE, HOSPITAL NAME Assignee, HOSPITAL REPRESENTATIVE, SIGNED, HAS AN ORIGINAL AUTHORIZATION OR, IS THE ORIGINAL SIGNATURE OF THE, NYS FORM NF Rev, YES, YES, AUTHORIZATION FOR RELEASE OF, THIS AUTHORIZATION OR PHOTOCOPY, and SIGNATURE PATIENT PARENT OR.
Those who use this PDF generally make mistakes while filling in AUTHORIZATION FOR RELEASE OF in this area. You need to go over everything you enter right here.
Step 3: Always make sure that the information is accurate and just click "Done" to continue further. Join FormsPal now and immediately obtain nf5 form fillable, all set for download. All alterations you make are preserved , meaning you can modify the form at a later point anytime. FormsPal guarantees your data privacy by using a protected system that never records or distributes any kind of personal information typed in. Feel safe knowing your files are kept safe each time you work with our services!