The MassHealth Buy-In program offers a critical financial resource for Massachusetts residents eligible for Medicare. It functions under congressional authorization, aiming to alleviate the financial burden of Medicare Part B premiums for those who might not avail of other MassHealth benefits. This program is particularly advantageous for individuals or couples living on a fixed income, as it imposes specific income and asset thresholds to determine eligibility. Beyond covering Part B premiums, the program extends its benefits to enable enrollees who have only Medicare Part A to obtain Part B coverage, thus broadening their access to comprehensive healthcare. Eligibility determination hinges on the submission of a Buy In Application, which requires detailed financial information and mandates that applicants adhere to specified income and asset limits. Once approved, participants will notice an increase in their social security checks, reflecting the no longer deducted Medicare Part B premium, or MassHealth will directly pay their Part B premiums if these were previously settled through alternative means. Coverage initiation is retroactive to the application month, potentially extending to three months before the application, ensuring that eligible individuals do not endure undue financial strain. The program also emphasizes confidentiality, fairness in treatment, and provides an avenue for appeals, underscoring its commitment to equitable access to healthcare. Additionally, it offers the possibility of appointing an authorized representative to streamline the application process, ensuring that all potential barriers to enrollment are minimized. This comprehensive approach not only aids in covering costs associated with Medicare Part B but also reinforces the broader objectives of MassHealth in supporting residents' healthcare needs.
| Question | Answer |
|---|---|
| Form Name | Buy In Application Form |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | mashealth buy in application, masshealth buy in online, masshealth state buy in program, masshealth buy in |
for people who are eligible for Medicare
What is MassHealth
MassHealth
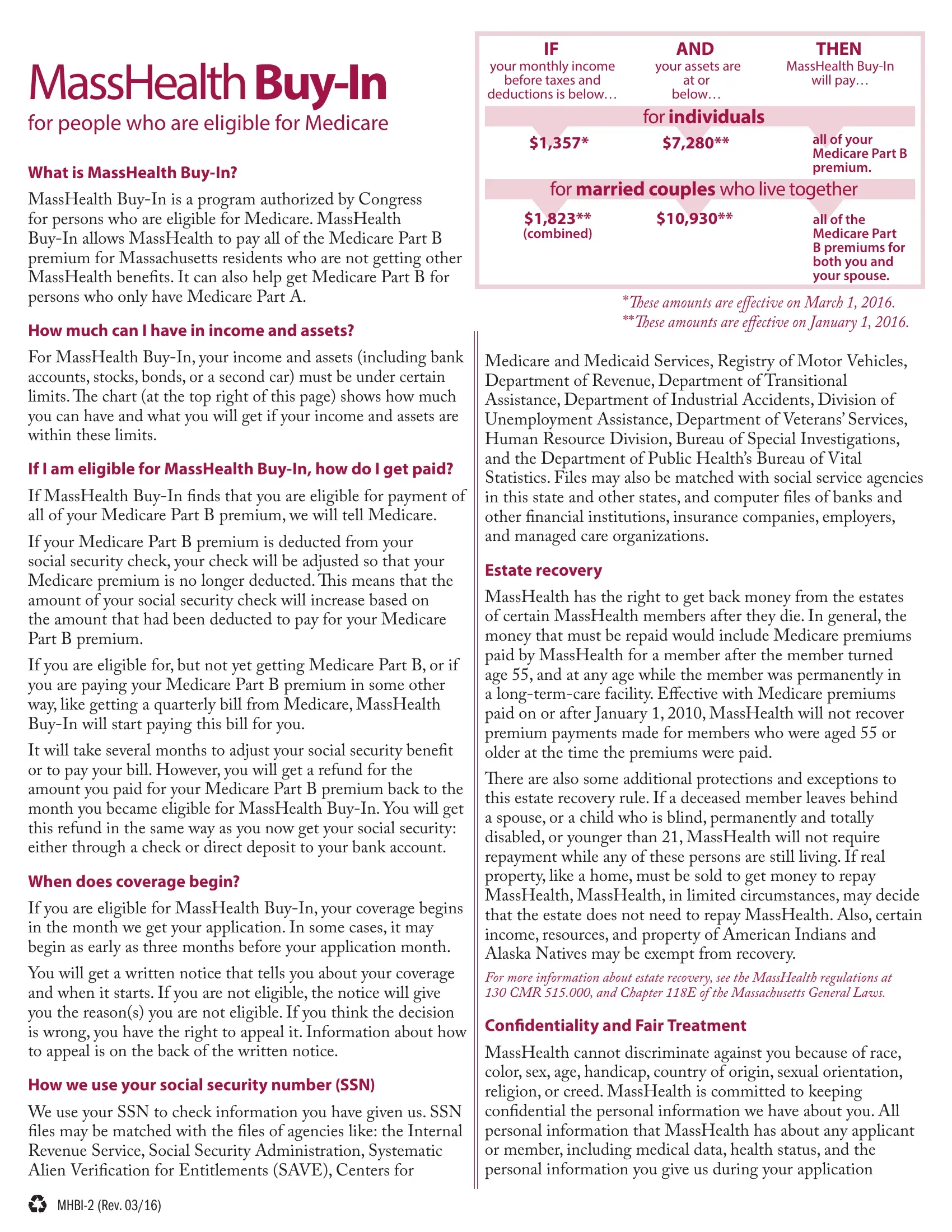
How much can I have in income and assets?
For MassHealth
If I am eligible for MassHealth
If MassHealth
If your Medicare Part B premium is deducted from your social security check, your check will be adjusted so that your Medicare premium is no longer deducted. his means that the amount of your social security check will increase based on the amount that had been deducted to pay for your Medicare Part B premium.
If you are eligible for, but not yet getting Medicare Part B, or if you are paying your Medicare Part B premium in some other way, like getting a quarterly bill from Medicare, MassHealth
It will take several months to adjust your social security beneit or to pay your bill. However, you will get a refund for the amount you paid for your Medicare Part B premium back to the month you became eligible for MassHealth
When does coverage begin?
If you are eligible for MassHealth
You will get a written notice that tells you about your coverage and when it starts. If you are not eligible, the notice will give you the reason(s) you are not eligible. If you think the decision is wrong, you have the right to appeal it. Information about how to appeal is on the back of the written notice.
How we use your social security number (SSN)
We use your SSN to check information you have given us. SSN iles may be matched with the iles of agencies like: the Internal Revenue Service, Social Security Administration, Systematic Alien Veriication for Entitlements (SAVE), Centers for
IF |
AND |
THEN |
your monthly income |
your assets are |
MassHealth |
before taxes and |
at or |
will pay… |
deductions is below… |
below… |
|
|
for individuals |
|
$1,357* |
$7,280** |
all of your |
|
|
Medicare Part B |
|
|
premium. |
for married couples who live together |
||
$1,823** |
$10,930** |
all of the |
(combined) |
|
Medicare Part |
|
|
B premiums for |
|
|
both you and |
|
|
your spouse. |
|
|
|
*hese amounts are efective on March 1, 2016. **hese amounts are efective on January 1, 2016.
Medicare and Medicaid Services, Registry of Motor Vehicles, Department of Revenue, Department of Transitional Assistance, Department of Industrial Accidents, Division of Unemployment Assistance, Department of Veterans’ Services, Human Resource Division, Bureau of Special Investigations, and the Department of Public Health’s Bureau of Vital Statistics. Files may also be matched with social service agencies in this state and other states, and computer iles of banks and other inancial institutions, insurance companies, employers, and managed care organizations.
Estate recovery
MassHealth has the right to get back money from the estates of certain MassHealth members after they die. In general, the money that must be repaid would include Medicare premiums paid by MassHealth for a member after the member turned age 55, and at any age while the member was permanently in a
here are also some additional protections and exceptions to this estate recovery rule. If a deceased member leaves behind a spouse, or a child who is blind, permanently and totally disabled, or younger than 21, MassHealth will not require repayment while any of these persons are still living. If real property, like a home, must be sold to get money to repay MassHealth, MassHealth, in limited circumstances, may decide that the estate does not need to repay MassHealth. Also, certain income, resources, and property of American Indians and Alaska Natives may be exempt from recovery.
For more information about estate recovery, see the MassHealth regulations at 130 CMR 515.000, and Chapter 118E of the Massachusetts General Laws.
Conidentiality and Fair Treatment
MassHealth cannot discriminate against you because of race, color, sex, age, handicap, country of origin, sexual orientation, religion, or creed. MassHealth is committed to keeping conidential the personal information we have about you. All personal information that MassHealth has about any applicant or member, including medical data, health status, and the personal information you give us during your application
for and receipt of beneits is conidential. his information may not be used or released for purposes other than the administration of MassHealth without your permission, unless required by law or a court order. You can give us your written permission to use your personal health information for a speciic purpose or to share it with a speciic person or organization.
Authorized Representative
An authorized representative is someone you choose to help you get health care coverage through programs ofered by MassHealth and the Massachusetts Health Connector. You can do this by illing out the Authorized Representative Designation Form (ARD) or a similar designation form. An authorized representative may ill out your application or eligibility review forms, give proof of information given on these eligibility forms, report changes in your income, address, or other circumstances, get copies of all MassHealth or Health Connector eligibility or enrollment notices sent to you, and act on your behalf in all other matters with MassHealth or the Health Connector.
An authorized representative can be a friend, family member, relative, or other person or organization of your choosing who agrees to help you. It is up to you to choose an authorized representative, if you want one. MassHealth or the Health Connector will not choose an authorized representative for you.
You must designate in writing on the Authorized Representative Designation Form or a similar designation document or authorization document the person or organization you want to be your authorized representative. In most cases, your authorized representative must also ill out this form or a similar designation document or authorization document. his form is included in the application packet, or you can call us or visit www.mass.gov/masshealth to get one. Please see the instructions on the form for more details.
An authorized representative can also be someone who is acting responsibly on your behalf if you cannot designate an authorized representative in writing because of a mental or physical condition, or has been appointed by law to act on your behalf or on behalf of your estate. his person must ill out the applicable parts of the Authorized Representative Designation Form or provide a similar designation document. If this person has been appointed by law to represent you, either you or this person must also submit to MassHealth or the Health Connector a copy of the applicable legal document stating that this person is lawfully representing you or your estate. his person may be a legal guardian, conservator, holder of power of attorney, or health care proxy, or if the applicant or member has died, the estate’s administrator or executor.
Permission to Share Information
If you want us to share your personal health information, including sending copies of your eligibility notices, with someone who is not your authorized representative, you can do this by giving us written permission. We have forms you can use to do this. You can call us or visit www.mass.gov/ masshealth to get a copy of the appropriate form.
Reporting Changes
If there are any changes in your income, assets, address, health insurance, immigration status, or disability status, you must tell us within 10 calendar days of the changes or as soon
as possible. If you do not tell us about these changes, you may lose your beneits. You can tell us about any changes by calling
Other MassHealth beneits
MassHealth ofers other health care beneits that either pay for medical services directly, or pay your Medicare copayments and deductibles. You may be eligible for these beneits if your income and assets are under certain amounts, or if you are disabled and younger than 65. Call a MassHealth Enrollment Center at
Other beneits
Medicare recipients can get help with prescription drug costs through Medicare. To get more information, call Medicare at
he Executive Oice of Elder Afairs also ofers help with prescription drug costs through Prescription Advantage. Call Elder Afairs toll free at
How do I apply for MassHealth
1.To apply for MassHealth
2.Sign the
send it to: MassHealth Enrollment Center Central Processing Unit
P.O. Box 290794 Charlestown, MA
or fax it to:
3.When we get the application, we will review it for completeness. If we need more information, we will write to you or call. Once we get all information, we will decide if you are eligible. We will also decide if your spouse is eligible.
4.A voter registration form is included with your application. (You do not need to register to vote to get MassHealth
5.If you want someone to act on your behalf as your authorized representative, use the enclosed Authorized Representative Designation Form to tell us.
(CUT ON THE DOTTED LINE)

MassHealth
Commonwealth of Massachusetts
EOHHS
www.mass.gov/masshealth
for people who are eligible for Medicare
This is an application for payment of your Medicare Part B premium. It can also help you get Medicare Part B if you are only getting Medicare Part A. If you want to apply for other MassHealth beneits, call a MassHealth Enrollment Center at
General Information
Who is applying? you
you and your spouse
If you and your spouse live together, you must also give us information about your spouse even if he or she is not applying for beneits.
YOU
|
Last name |
|
|
|
|
|
|
First name |
|
|
MI |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Street address |
|
|
|
|
|
|
City |
|
State |
Zip |
|
|
|
|
|
|
|
|
|
|
|
|||
|
Mailing address (if diferent from above) homeless |
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
City |
|
State |
Zip |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date of birth |
/ |
/ |
Gender |
M |
F |
Preferred written language |
Telephone number ( |
|
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Social security number |
|
|
|
For oice use only |
Medicare claim number |
|
For oice use only |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
YOUR SPOUSE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Last name |
|
|
|
|
|
|
First name |
|
|
MI |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date of birth |
/ |
/ |
Gender |
M |
F |
Preferred written language |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Social security number |
|
|
|
For oice use only |
Medicare claim number |
|
For oice use only |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Income
Fill out this section for you and your spouse. List the gross monthly income (before taxes and other deductions, such as the Medicare Part B premium). Send proof of your income, like a copy of a recent paystub or pension check stub. (You do not have to send proof of social security income.)
|
Source of income |
|
Your gross monthly income |
|
Your spouse’s gross monthly income |
|||
|
|
before taxes and deductions |
|
before taxes and deductions |
||||
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
Social security |
$ |
|
For oice use only |
$ |
|
For oice use only |
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
Pensions |
$ |
|
|
$ |
|
|
|
|
|
|
|
|
|
|
|
|
|
Veterans’ beneits |
$ |
|
|
$ |
|
|
|
|
|
|
|
|
|
|
|
|
|
Annuities or trusts |
$ |
|
|
$ |
|
|
|
|
|
|
|
|
|
|
|
|
|
Dividends and/or interest |
$ |
|
|
$ |
|
|
|
|
|
|
|
|
|
|
|
|
|
Income from a job (before deductions) |
$ |
|
|
$ |
|
|
|
|
|
|
|
|
|
|
|
|
|
Rental income (after expenses) |
$ |
|
|
$ |
|
|
|
|
|
|
|
|
|
|
|
|
|
Other (please specify) |
$ |
|
|
$ |
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 |
|
|
over |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
||
Assets
|
|
Source |
|
You |
|
Your spouse |
|
You and your spouse |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Savings accounts |
$ |
|
|
$ |
|
|
$ |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Checking accounts |
$ |
|
|
$ |
|
|
$ |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Second car |
$ |
|
|
$ |
|
|
$ |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Certiicates of deposit |
$ |
|
|
$ |
|
|
$ |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Stocks |
$ |
|
|
$ |
|
|
$ |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Bonds |
$ |
|
|
$ |
|
|
$ |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Mutual funds |
$ |
|
|
$ |
|
|
$ |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Other (please specify) |
$ |
|
|
$ |
|
|
$ |
|
|
||
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Total assets |
$ |
|
For oice use only |
$ |
|
For oice use only |
$ |
|
For oice use only |
||
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Signature
Please read the following carefully. Then sign and date the bottom of this page. Both you and your spouse must sign if your spouse lives with you.
I give permission to MassHealth to get any records or data to prove any information given on this application. I understand that I must tell MassHealth of any changes in information I gave on this application. I further certify under the penalty of perjury that the information on this application is correct and complete to the best of my knowledge.
If you are acting on behalf of someone in filling out this application, the enclosed Authorized Representative Designation Form must also be filled out and sent back with this application. Your signature on this application as an authorized representative certifies that the information on this application is correct and complete to the best of your knowledge.
If you think MassHealth’s decision about whether you are eligible is wrong, you have the right to appeal. If you are denied benefits, you will get information on how to appeal.
X
Signature of applicant or authorized representativePrint nameDate
X
Signature of applicant’s spouse or authorized representative |
Print name |
Date |
Once you have filled out and signed this form,
send it to:
MassHealth Enrollment Center
Central Processing Unit
P.O. Box 290794
Charlestown, MA
OR
fax it to:
2