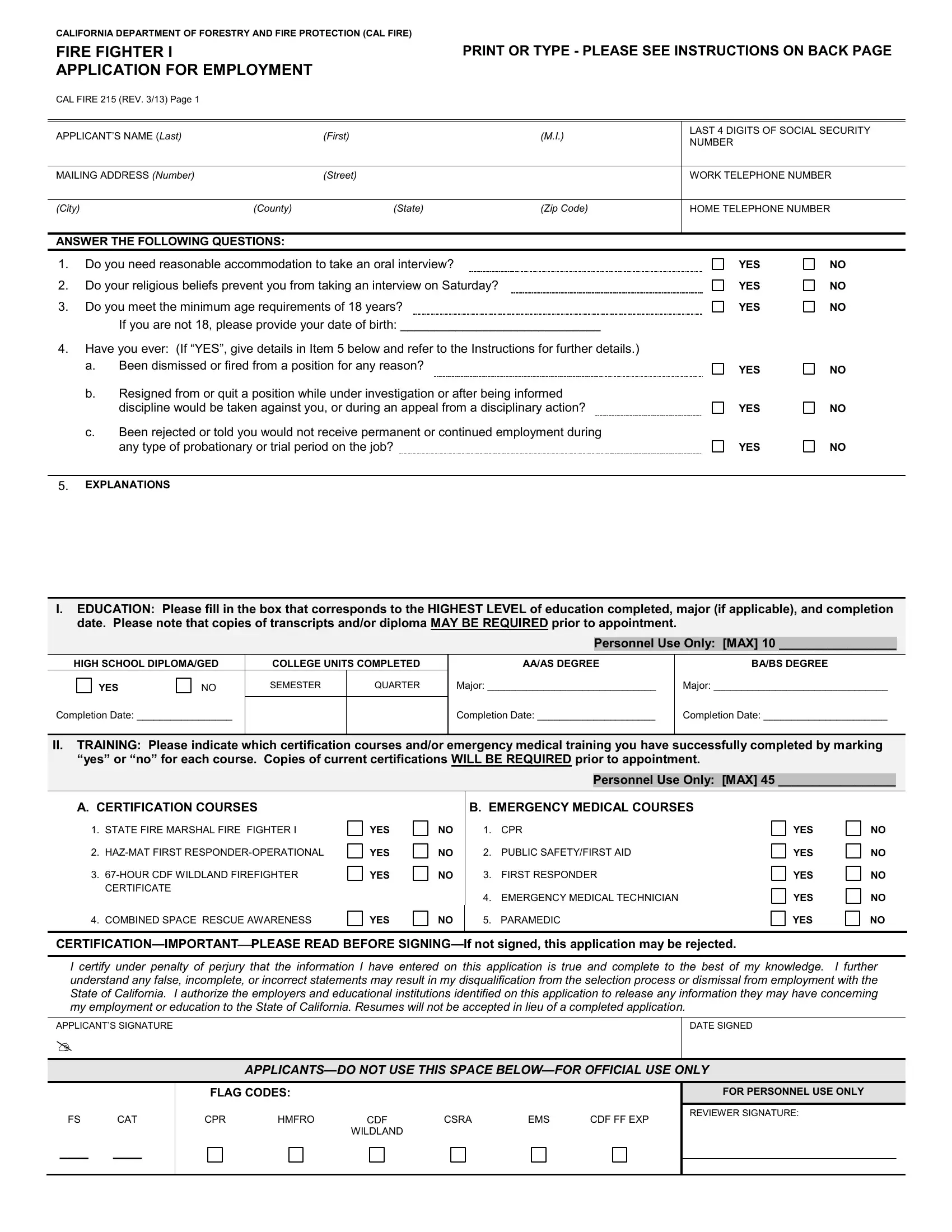
The Cal Fire 215 form serves as a comprehensive application for employment within the California Department of Forestry and Fire Protection (CAL FIRE) for the position of Fire Fighter I. It requires applicants to provide detailed personal information, including the last four digits of their Social Security Number, contact information, and answers to preliminary screening questions such as the need for reasonable accommodation during the interview process, religious beliefs affecting interview scheduling, and minimum age requirements. The form extends into thorough inquiries about the applicant's education, including the highest level of education completed, training certifications particularly relevant to firefighting and emergency medical services, as well as explicit listings of both firefighting and non-firefighting work experience. Applicants are asked to list their jobs, including the role, employer, and duration for various categories like CDF firefighting experience, non-CDF firefighting experience, volunteer or reserve firefighting experience, public safety, medical care provider roles, and trades or industrial experience. This meticulous documentation is designed to capture a wide range of information to evaluate candidates’ qualifications and readiness for the demanding role of a Fire Fighter I. To ensure accuracy and honesty, the form culminates with a certification that all information provided is true, under penalty of perjury, and permits the verification of such data from the listed employers and educational institutions. It’s clear that the Cal Fire 215 form plays a crucial role in the CAL FIRE hiring process, setting a high standard for candidate evaluation to maintain the department’s excellence in forest and fire protection.
| Question | Answer |
|---|---|
| Form Name | Cal Fire 215 Form |
| Form Length | 7 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min 45 sec |
| Other names | CALIFORNIA, responder, MDY, APPLICANTSDO |
CALIFORNIA DEPARTMENT OF FORESTRY AND FIRE PROTECTION (CAL FIRE)
FIRE FIGHTER I |
PRINT OR TYPE - PLEASE SEE INSTRUCTIONS ON BACK PAGE |
APPLICATION FOR EMPLOYMENT |
|
CAL FIRE 215 (REV. 3/13) Page 1 |
|
APPLICANT’S NAME (Last) |
(First) |
(M.I.) |
LAST 4 DIGITS OF SOCIAL SECURITY NUMBER
MAILING ADDRESS (Number) |
(Street) |
WORK TELEPHONE NUMBER
(City) |
(County) |
(State) |
(Zip Code) |
HOME TELEPHONE NUMBER
ANSWER THE FOLLOWING QUESTIONS:
1. |
Do you need reasonable accommodation to take an oral interview? |
YES |
NO |
2. |
Do your religious beliefs prevent you from taking an interview on Saturday? |
YES |
NO |
3. |
Do you meet the minimum age requirements of 18 years? |
YES |
NO |
|
If you are not 18, please provide your date of birth: _____________________________ |
|
|
4.Have you ever: (If “YES”, give details in Item 5 below and refer to the Instructions for further details.)
a. |
Been dismissed or fired from a position for any reason? |
YES |
NO |
|
|
b. |
Resigned from or quit a position while under investigation or after being informed |
|
|
|
discipline would be taken against you, or during an appeal from a disciplinary action? |
YES |
NO |
c.Been rejected or told you would not receive permanent or continued employment during
any type of probationary or trial period on the job? |
YES |
NO |
5.EXPLANATIONS
I.EDUCATION: Please fill in the box that corresponds to the HIGHEST LEVEL of education completed, major (if applicable), and completion date. Please note that copies of transcripts and/or diploma MAY BE REQUIRED prior to appointment.
Personnel Use Only: [MAX] 10 _________________
HIGH SCHOOL DIPLOMA/GED |
COLLEGE UNITS COMPLETED |
||
YES |
NO |
SEMESTER |
QUARTER |
AA/AS DEGREE |
BA/BS DEGREE |
Major: ______________________________ |
Major: _______________________________ |
Completion Date: _________________
Completion Date: _____________________ |
Completion Date: ______________________ |
II.TRAINING: Please indicate which certification courses and/or emergency medical training you have successfully completed by marking ―yes‖ or ―no‖ for each course. Copies of current certifications WILL BE REQUIRED prior to appointment.
Personnel Use Only: [MAX] 45 _________________
A.CERTIFICATION COURSES
1.STATE FIRE MARSHAL FIRE FIGHTER I
2.
3.
4.COMBINED SPACE RESCUE AWARENESS
YES
YES YES
YES
NO
NO NO
NO
B.EMERGENCY MEDICAL COURSES
1.CPR
2.PUBLIC SAFETY/FIRST AID
3.FIRST RESPONDER
4.EMERGENCY MEDICAL TECHNICIAN
5.PARAMEDIC
YES
YES
YES
YES
YES
NO
NO
NO
NO
NO
I certify under penalty of perjury that the information I have entered on this application is true and complete to the best of my knowledge. I further understand any false, incomplete, or incorrect statements may result in my disqualification from the selection process or dismissal from employment with the State of California. I authorize the employers and educational institutions identified on this application to release any information they may have concerning my employment or education to the State of California. Resumes will not be accepted in lieu of a completed application.
APPLICANT’S SIGNATURE
DATE SIGNED
FS CAT
___ ___
FLAG CODES:
CPR |
HMFRO |
CDF |
CSRA |
EMS |
CDF FF EXP |
|
|
WILDLAND |
|
|
|
FOR PERSONNEL USE ONLY
REVIEWER SIGNATURE:
CALIFORNIA DEPARTMENT OF FORESTRY AND FIRE PROTECTION (CAL FIRE)
FIRE FIGHTER I |
PRINT OR TYPE - PLEASE SEE INSTRUCTIONS ON BACK PAGE |
APPLICATION FOR EMPLOYMENT |
|
CAL FIRE 215 (REV. 3/13) Page 2 |
|
APPLICANT’S NAME (Last) |
(First) |
(M.I.) |
LAST 4 DIGITS OF SOCIAL SECURITY NUMBER
III.FIREFIGHTING EXPERIENCE: List the applicable information specified below including classification title, location, employer, and
|
months of experience. ALL INFORMATION WILL BE VERIFIED PRIOR TO APPOINTMENT. |
[MAX] 30 _________________ |
|
|
|
|
|
A). CDF FIREFIGHTING EXPERIENCE
Include CDF firefighting experience only (i.e., Fire Fighter I, Conservation Camp, Fire Center)
FROM (MDY) |
TO (MDY) |
JOB TITLE/CLASSIFICATION (Include Range or Level, If applicable) |
|
|
|
HOURS PER WEEK |
TOTAL WORKED (Years/Months) |
CDF UNIT |
|
|
|
SALARY EARNED |
|
ADDRESS |
$ |
PER |
|
DUTIES PERFORMED |
|
|
REASON FOR LEAVING |
|
|
|
|
|
FROM (MDY) |
TO (MDY) |
JOB TITLE/CLASSIFICATION (Include Range or Level, If applicable) |
|
|
|
HOURS PER WEEK |
TOTAL WORKED (Years/Months) |
CDF UNIT |
|
|
|
SALARY EARNED |
|
ADDRESS |
$ |
PER |
|
DUTIES PERFORMED |
|
|
REASON FOR LEAVING
B.)
Include
FROM (MDY) |
TO (MDY) |
JOB TITLE/CLASSIFICATION (Include Range or Level, If applicable) |
|
|
|
HOURS PER WEEK |
TOTAL WORKED (Years/Months) |
COMPANY/STATE AGENCY NAME |
|
|
|
SALARY EARNED |
|
ADDRESS |
$ |
PER |
|
DUTIES PERFORMED |
|
|
REASON FOR LEAVING
CALIFORNIA DEPARTMENT OF FORESTRY AND FIRE PROTECTION (CAL FIRE)
FIRE FIGHTER I |
PRINT OR TYPE - PLEASE SEE INSTRUCTIONS ON BACK PAGE |
APPLICATION FOR EMPLOYMENT |
|
CAL FIRE 215 (REV. 3/13) Page 3 |
|
APPLICANT’S NAME (Last) |
(First) |
(M.I.) |
LAST 4 DIGITS OF SOCIAL SECURITY NUMBER
III. FIREFIGHTING EXPERIENCE, CONTINUED:
B.)
Include
FROM (MDY) |
TO (MDY) |
JOB TITLE/CLASSIFICATION (Include Range or Level, If applicable) |
|
|
|
HOURS PER WEEK |
TOTAL WORKED (Years/Months) |
COMPANY/STATE AGENCY NAME |
|
|
|
SALARY EARNED |
|
ADDRESS |
$ |
PER |
|
DUTIES PERFORMED |
|
|
REASON FOR LEAVING
C.) PAID CALL, VOLUNTEER AND/OR RESERVE FIREFIGHTING EXPERIENCE
Include firefighting experience gained as a Paid Call, Volunteer, and or Reserve Fire Fighter and/or CDF Emergency Worker or Fire Fighter Explorer
FROM (MDY) |
TO (MDY) |
JOB TITLE/CLASSIFICATION (Include Range or Level, If applicable) |
|
|
|
HOURS PER WEEK |
TOTAL WORKED (Years/Months) |
COMPANY/STATE AGENCY NAME |
|
|
|
SALARY EARNED |
|
ADDRESS |
$ |
PER |
|
DUTIES PERFORMED |
|
|
REASON FOR LEAVING
FROM (MDY) |
TO (MDY) |
JOB TITLE/CLASSIFICATION (Include Range or Level, If applicable) |
|
|
|
HOURS PER WEEK |
TOTAL WORKED (Years/Months) |
COMPANY/STATE AGENCY NAME |
|
|
|
SALARY EARNED |
ADDRESS |
COMPANY/STATE AGENCY NAME |
$ |
PER |
|
DUTIES PERFORMED |
|
|
REASON FOR LEAVING
CALIFORNIA DEPARTMENT OF FORESTRY AND FIRE PROTECTION (CAL FIRE)
FIRE FIGHTER I |
PRINT OR TYPE - PLEASE SEE INSTRUCTIONS ON BACK PAGE |
APPLICATION FOR EMPLOYMENT |
|
CAL FIRE 215 (REV. 3/13) Page 4 |
|
APPLICANT’S NAME (Last) |
(First) |
(M.I.) |
LAST 4 DIGITS OF SOCIAL SECURITY NUMBER
IV.
|
months of experience. ALL INFORMATION WILL BE VERIFIED PRIOR TO APPOINTMENT. |
[MAX] 15 _________________ |
|
|
|
|
|
A.) PUBLIC SAFETY
Include work experience in a public safety area of AT LEAST 6 MONTHS DURATION (i.e., CDF Volunteers in Prevention, Military, Security Guard, Lifeguard, Dispatcher, Park Ranger)
FROM (MDY) |
TO (MDY) |
JOB TITLE/CLASSIFICATION (Include Range or Level, If applicable) |
|
|
|
HOURS PER WEEK |
TOTAL WORKED (Years/Months) |
COMPANY/STATE AGENCY NAME |
|
|
|
SALARY EARNED |
|
ADDRESS |
$ |
PER |
|
DUTIES PERFORMED |
|
|
REASON FOR LEAVING
B.) MEDICAL CARE PROVIDER
Include work experience as a medical care provider of AT LEAST 6 MONTHS DURATION. Experience must include direct patient care (i.e., Ambulance Attendant, Emergency Room Technician). Do NOT include
FROM (MDY) |
TO (MDY) |
JOB TITLE/CLASSIFICATION (Include Range or Level, If applicable) |
|
|
|
HOURS PER WEEK |
TOTAL WORKED (Years/Months) |
COMPANY/STATE AGENCY NAME |
|
|
|
SALARY EARNED |
|
ADDRESS |
$ |
PER |
|
|
|
|
DUTIES PERFORMED |
|
|
REASON FOR LEAVING
FROM (MDY) |
TO (MDY) |
JOB TITLE/CLASSIFICATION (Include Range or Level, If applicable) |
|
|
|
HOURS PER WEEK |
TOTAL WORKED (Years/Months) |
COMPANY/STATE AGENCY NAME |
|
|
|
SALARY EARNED |
|
ADDRESS |
$ |
PER |
|
DUTIES PERFORMED |
|
|
REASON FOR LEAVING
CALIFORNIA DEPARTMENT OF FORESTRY AND FIRE PROTECTION (CAL FIRE)
FIRE FIGHTER I |
PRINT OR TYPE - PLEASE SEE INSTRUCTIONS ON BACK PAGE |
APPLICATION FOR EMPLOYMENT |
|
CAL FIRE 215 (REV. 3/13) Page 5 |
|
APPLICANT’S NAME (Last) |
(First) |
(M.I.) |
LAST 4 DIGITS OF SOCIAL SECURITY NUMBER
IV.
C.) TRADES/INDUSTRIAL/OTHER EXPERIENCE
Include trades/industrial experience of AT LEAST 6 MONTHS DURATION (i.e., Carpenter, Mechanic, Cook, etc.).
FROM (MDY) |
TO (MDY) |
JOB TITLE/CLASSIFICATION (Include Range or Level, If applicable) |
|
|
|
HOURS PER WEEK |
TOTAL WORKED (Years/Months) |
COMPANY/STATE AGENCY NAME |
|
|
|
SALARY EARNED |
|
ADDRESS |
$ |
PER |
|
DUTIES PERFORMED |
|
|
REASON FOR LEAVING |
|
|
|
|
|
FROM (MDY) |
TO (MDY) |
JOB TITLE/CLASSIFICATION (Include Range or Level, If applicable) |
|
|
|
HOURS PER WEEK |
TOTAL WORKED (Years/Months) |
COMPANY/STATE AGENCY NAME |
|
|
|
SALARY EARNED |
|
ADDRESS |
$ |
PER |
|
DUTIES PERFORMED |
|
|
REASON FOR LEAVING
FROM (MDY) |
TO (MDY) |
JOB TITLE/CLASSIFICATION (Include Range or Level, If applicable) |
|
|
|
HOURS PER WEEK |
TOTAL WORKED (Years/Months) |
COMPANY/STATE AGENCY NAME |
|
|
|
SALARY EARNED |
|
ADDRESS |
$ |
PER |
|
DUTIES PERFORMED |
|
|
REASON FOR LEAVING
NOTE: IF MORE SPACE IS NEEDED FOR EXPERIENCE, ATTACH ADDITIONAL PAGES.
CALIFORNIA DEPARTMENT OF FORESTRY AND FIRE PROTECTION (CDF)
FIRE FIGHTER I
APPLICATION FOR EMPLOYMENT
CDF 215 (REV. 3/13) Page 6
EQUAL EMPLOYMENT OPPORTUNITY
APPLICANT: To assist the State of California in its commitment to Equal Employment Opportunity, applicants are asked to voluntarily provide the following information. This questionnaire will be separated from the application prior to any employment decisions. Government Code Section 19705 authorizes the State Personnel Board to retain this information for research and statistical purposes.
AGE
UNDER 21
21- 39
GENDER
70 AND OVER |
|
MALE |
FEMALE
Ethnic Category (Please check the box that best describes your race/ethnicity):
AMERICAN INDIAN OR ALASKAN NATIVE - Persons having origins in any of the tribal peoples of North America, and who maintain cultural identification through tribal affiliation or community recognition.
ENTER TRIBAL IDENTIFICATION OR AFFILIATION:
ASIAN - Persons having origins in any of the original peoples of the Far East, Southeast Asia, or the Indian Subcontinent. This includes China, Japan, and Korea.
BLACK - Persons having origins in any of the black racial groups of Africa.
FILIPINO - Persons having origins in any of the original peoples of the Philippine Islands.
HISPANIC - Persons of Mexican, Puerto Rican, Central or South American, or other Spanish culture or origin, regardless of race.
PACIFIC ISLANDERS - Persons having origins in the Pacific Islands, such as Samoa.
WHITE - Persons having origins in any of the original peoples of Europe, North Africa, or the Middle East.
Check if:
OTHER (Specify)
DISABLED - A person with a disability is an individual who:
(1)Has a physical or mental impairment that substantially limits one or more life activities, such as walking, speaking, breathing, performing manual tasks, seeing, hearing, learning, caring for oneself or working;
(2)Has a record of such an impairment;
(3)Is regarded as having such impairment.
MILITARY - A military veteran; a widow or widower of a veteran; or a spouse of a 100% disabled veteran.
HOW DID YOU LEARN OF THE FIRE FIGHTER I POSITION?
NEWSPAPER |
RECRUITER |
JOB ANNOUNCEMENT |
SCHOOL |
INTERNET FRIEND/RELATIVE
OTHER (Specify) ___________________________
THANK YOU FOR COMPLETING THIS QUESTIONNAIRE
CALIFORNIA DEPARTMENT OF FORESTRY AND FIRE PROTECTION (CDF)
FIRE FIGHTER I
APPLICATION FOR EMPLOYMENT
CDF 215 (REV.
INSTRUCTIONS
Read the following instructions carefully before completing this Application. Please complete the Application on a typewriter or personal computer or print in ink. All questions must be answered completely and accurately, except as noted. You may be disqualified for any false or misleading statements or for omitting information. The information you furnish will be used to determine your eligibility and/or may be the basis for arriving at your final rating. You may be requested to provide additional information regarding your qualifications, your preference regarding work shifts, etc., and health/medical background.
Social Security Number – Please provide the last four (4) digits of your social security number.
Question 1 – Reasonable Accommodation will be
provided to applicants who need assistance to participate in an interview due to a verifiable disability. If you check “yes”
you will be contacted via telephone or mail to make specific arrangements.
Question 3 – The minimum age requirement for a Fire Fighter I is 18 years of age at the time of appointment. If you are not currently 18 years of age or older, please indicate your date of birth in the space provided.
Question 4 – Employment History/Discharges. These
questions must be answered by all applicants. (a) You must answer “yes” if you have ever, because of poor
performance or misconduct, been fired from a job, let go, or had a work contract terminated. (b) You must answer “yes”
if you have ever quit a job after being informed that you were under suspicion of misconduct or poor performance or after being informed you could receive disciplinary action.
(c)You must answer “yes” if you were ever advised that you would be rejected, released, or not hired permanently after a trial period. Explain any "yes" answers in Item 5. Include the facts in brief, the grounds for any action taken against you, and the circumstances under which you left the position.
SPECIAL NOTE: Verification of the items listed in Section I, Education and/or Section II, Training, may be required at the time of the interview or appointment. Acceptable verification for education is copies of your transcripts and/or diploma. The acceptable verification for training is a copy of your certificate of course completion and/or copy of both sides of your current, valid medical card.
Section I – Education. Fill in the highest level of education you have achieved and the date of completion. For college units, please indicate if semester or quarter units.
Section II – Training. Indicate all certification courses
and/or emergency medical training you have successfully completed by marking “yes” or “no.”
Signature – Your signature and the date signed is required. If the Application is not signed, it may be rejected and/or may result in your missing the final filing date for this application.
Section III – Firefighting Experience. You must include a complete list of your paid and/or volunteer firefighting work experience for the categories of: A.) CDF firefighting experience, B.)
Section IV –
State employees must list the specific departments for which they worked and indicate the specific civil service class title(s) held.
NOTE: Your completed Application and other related information submitted to CDF becomes confidential information and the property of the State of California as provided by Government Code Section 18934. This application and other confidential information will not be returned; therefore, we recommend that you keep a copy of your completed Application for your personal records.
Discrimination on the basis of race, color, creed, national origin, ancestry, sex, marital status, disability, religious our political affiliation, age, or sexual orientation is prohibited.
PLEASE ENTER YOUR NAME ON PAGES 1 THROUGH 5
AND STAPLE ALL PAGES OF THE
APPLICATION TOGETHER BEFORE SUBMITTING!