
mc 194 social administration can be filled out easily. Just make use of FormsPal PDF tool to do the job promptly. The tool is consistently improved by us, acquiring useful features and growing to be even more convenient. By taking a few simple steps, it is possible to start your PDF editing:
Step 1: Click on the "Get Form" button above. It will open up our tool so that you can start filling in your form.
Step 2: With our state-of-the-art PDF editor, you'll be able to accomplish more than just fill in forms. Express yourself and make your docs look sublime with custom text incorporated, or optimize the original content to excellence - all comes with an ability to incorporate almost any pictures and sign the PDF off.
For you to complete this document, make certain you provide the right details in every field:
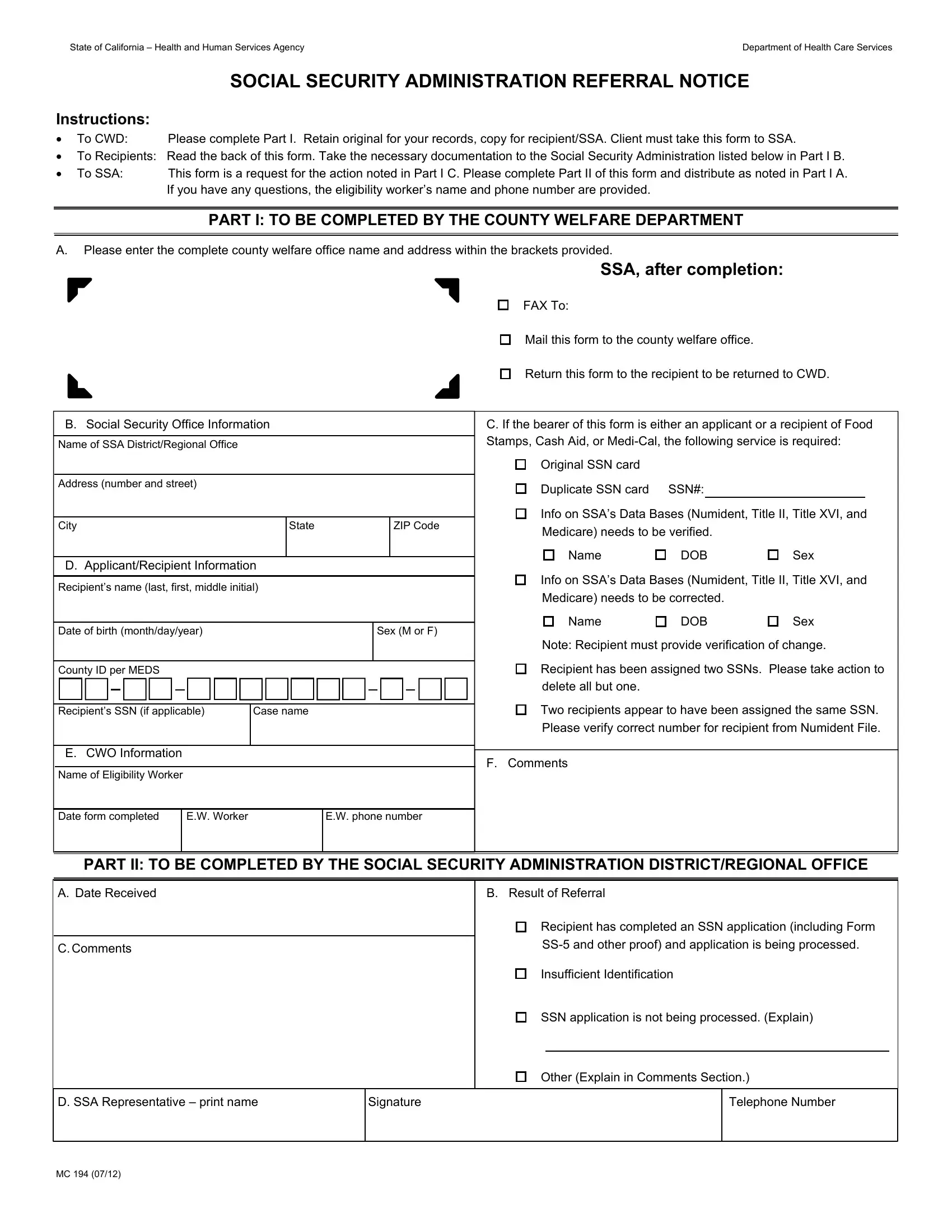
1. Complete the mc 194 social administration with a number of necessary fields. Gather all the required information and make certain there is nothing left out!
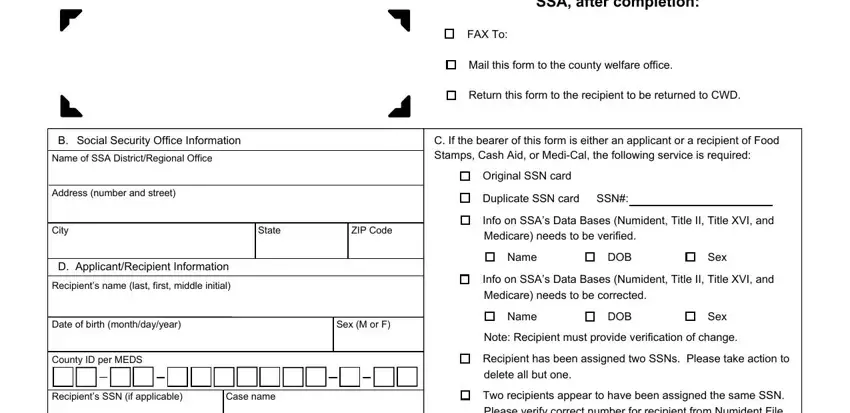
2. Once your current task is complete, take the next step – fill out all of these fields - F Comments, E CWO Information Name of, Date form completed, EW Worker, EW phone number, PART II TO BE COMPLETED BY THE, A Date Received, C Comments, D SSA Representative print name, MC , B Result of Referral, Recipient has completed an SSN, SS and other proof and application, Insufficient Identification, and SSN application is not being with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
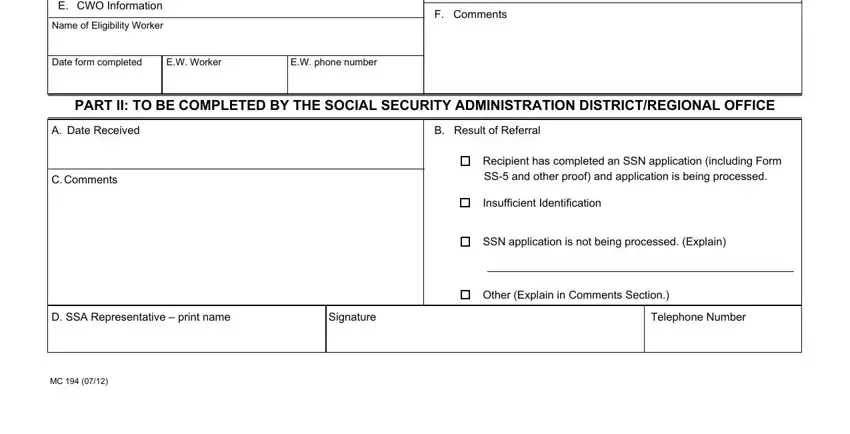
It's simple to make an error while completing the EW Worker, and so you'll want to take another look before you'll finalize the form.
Step 3: Make certain your details are correct and then press "Done" to proceed further. Join us today and immediately use mc 194 social administration, ready for download. All changes made by you are saved , helping you to edit the document at a later point if required. At FormsPal, we do everything we can to be sure that your information is maintained secure.