In the realm of personal health information, particularly within the mental health sector, the meticulous process of sharing such sensitive data requires a comprehensive understanding and adherence to both legal and ethical standards. The State of California, recognizing the delicate nature of mental health information and the need for stringent protections, has established the California MH 5671 form, employed by the Health and Human Services Agency Department of Mental Health. This pivotal document facilitates the authorized release of confidential patient information, adhering strictly to the guidelines set forth by the Welfare & Institutions Code Section 5328 and reinforced under the Health Insurance Portability and Accountability Act (HIPAA) Privacy Rule, specified in CFR Section 164.508. The form is crafted to ensure that the release of information does not occur without the explicit consent of the patient, or, when applicable, their parent, guardian, or conservator. With sections dedicated to specifying the nature of the information to be disclosed, the purposes for such disclosure, and strict timeliness for the authorization's validity, it underscores the patient's autonomy over their personal information, while simultaneously upholding the necessity for such data in facilitating their treatment, evaluation, or other pertinent reasons. Moreover, it emphasizes the non-contingency of treatment upon the signing of this authorization, the patient's right to refuse to sign, and the conditions under which information might still be released as required by law. Integral to this process is not just the agreement from the patient or their representative, but the attestation of a witness to the signing, ensuring an additional layer of verification and consent.
| Question | Answer |
|---|---|
| Form Name | California Form Mh 5671 |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names |
State of California - Health and Human Services Agency |
Department of Mental Health |
|
AUTHORIZATION FOR RELEASE |
Confidential Patient Information |
|
OF PATIENT INFORMATION |
See W&I Code Section 5328 and |
|
MH 5671 (Rev. 06/08) Page 1 of 3 |
HIPAA Privacy Rule CFR Section 164.508 |
|
___ |
|
___ |
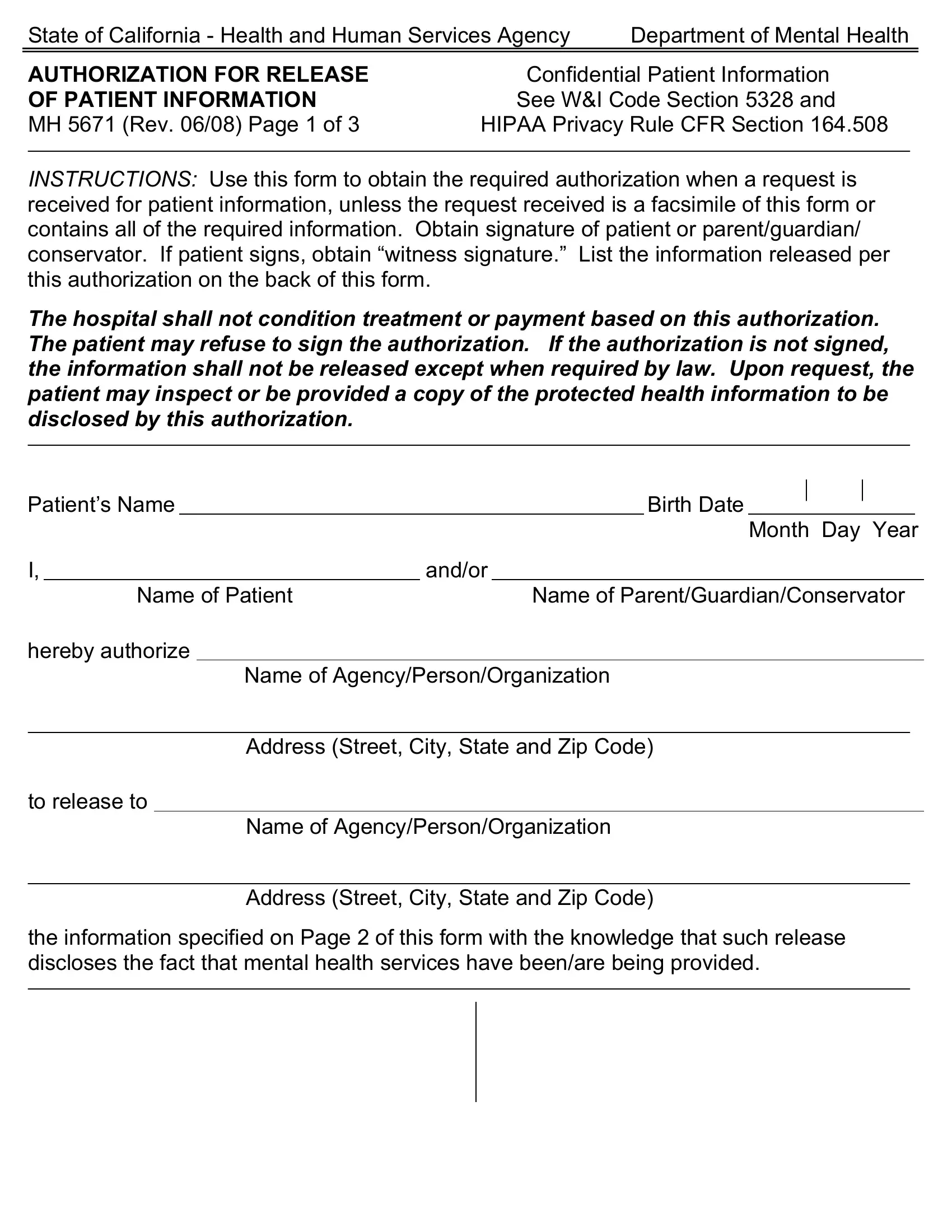
INSTRUCTIONS: Use this form to obtain the required authorization when a request is received for patient information, unless the request received is a facsimile of this form or contains all of the required information. Obtain signature of patient or parent/guardian/ conservator. If patient signs, obtain “witness signature.” List the information released per this authorization on the back of this form.
The hospital shall not condition treatment or payment based on this authorization. The patient may refuse to sign the authorization. If the authorization is not signed, the information shall not be released except when required by law. Upon request, the patient may inspect or be provided a copy of the protected health information to be disclosed by this authorization.
______
Patient’s Name |
|
|
|
Birth Date |
|
|
|
|
|
|
|
______________ |
|
||||||
|
|
|
|
|
|
Month Day Year |
|||
I, |
and/or |
|
|
|
|
||||
|
Name of Patient |
|
Name of Parent/Guardian/Conservator |
||||||
hereby authorize
Name of Agency/Person/Organization
___ |
___ |
Address (Street, City, State and Zip Code)
to release to
Name of Agency/Person/Organization
___ |
___ |
Address (Street, City, State and Zip Code)
the information specified on Page 2 of this form with the knowledge that such release discloses the fact that mental health services have been/are being provided.
___ |
___ |
State of California - Health and Human Services Agency |
Department of Mental Health |
|
AUTHORIZATION FOR RELEASE |
Confidential Patient Information |
|
OF PATIENT INFORMATION |
See W&I Code Section 5328 and |
|
MH 5671 (Rev. 06/08) Page 2 of 3 |
HIPAA Privacy Rule C.F.R. Section 164.508 |
|
___ |
|
___ |
This disclosure of information* is required for the following purpose(s): (initial applicable
areas) |
Evaluation |
Treatment Planning/Course |
Other (Specify) __________ |
and shall be limited to releasing the following types of information (initial all applicable areas): from (date required) __________________to (date required) __________________;
or any information/records indicated, regardless of date.
Entire Record
Diagnosis
Psychiatric Evaluation
Discharge Summary
Social History
Individual Treatment
Plan
Legal Information
Medical, Neurological
Assessment, Lab Tests,
e.g., EEG, EKG, etc.
Seclusion and/Restraint Information
HIV Tests Results
Other Evaluations/ Assessments (specify)
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
Results of Psychological/ Vocational Testing Conference(s) Date(s)
____________________
____________________
____________________
Other (specify)
____________________
____________________
____________________
____________________
*The information disclosure under this authorization may be subject to
(Month/Day/Year) ___. This authorization may be revoked in writing by the
undersigned at anytime except to the extent that action has already been taken. If not
revoked, it shall terminate at the end of (check one): |
6 months |
One year or |
Specify Date ____________________. |
|
|
I understand that I am to receive a copy of this authorization.
|
|
|
Date: |
|
|
|
|
|
|
|
|
|
|||
Signature of Patient |
|
|
|
|
Month |
Day |
Year |
|
|
|
Date: |
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|||
Signature of Parent/Guardian/Conservator, if Applicable |
Month |
Day |
Year |
||||
|
|
|
Date: |
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|||
Witness Signature |
|
|
|
|
Month |
Day |
Year |
|
|
|
|
||||
Signature of Professional* |
Date |
|
Person Obtaining Authorization Date |
||||
*Professional for this authorization refers only to a Physician, Licensed Psychologist or Social Worker with a Master’s degree in social work, or Marriage and Family Therapist who approves this patient initiated request for release of patient records.
State of California - Health and Human Services Agency |
Department of Mental Health |
|
AUTHORIZATION FOR RELEASE |
Confidential Patient Information |
|
OF PATIENT INFORMATION |
See W&I Code Section 5328 and |
|
MH 5671 (Rev. 06/08) Page 3 of 3 |
HIPAA Privacy Rule C.F.R. Section 164.508 |
|
___ |
|
___ |
RECORD OF RELEASE OF INFORMATION
The following information was released to the named party specified on the front of this form. Identify the specific dates of the reports, records, items released.
Entire Record
Diagnosis
Psychiatric Evaluation
Discharge Summary
Social History
Individual Treatment Plan
Other:
Legal Information
Medical, Neurological Assessment, Lab Tests, e.g., EEG, EKG, etc.
HIV Tests Results
Results of Psychological/ Vocational Testing
Other Evaluations/ Assessments (specify)
____________________
____________________
____________________
____________________
Conference(s) Date(s)
____________________
____________________
____________________
Released By (Name & Title) |
Date Released |
|
|