



Dealing with PDF forms online is certainly easy using our PDF tool. Anyone can fill out 295 application social here and try out many other functions available. The tool is continually upgraded by our staff, acquiring powerful functions and growing to be better. It merely requires just a few basic steps:
Step 1: Hit the "Get Form" button above on this page to get into our editor.
Step 2: The editor helps you modify most PDF forms in various ways. Modify it by adding your own text, correct original content, and include a signature - all at your fingertips!
With regards to the fields of this precise document, here is what you should consider:
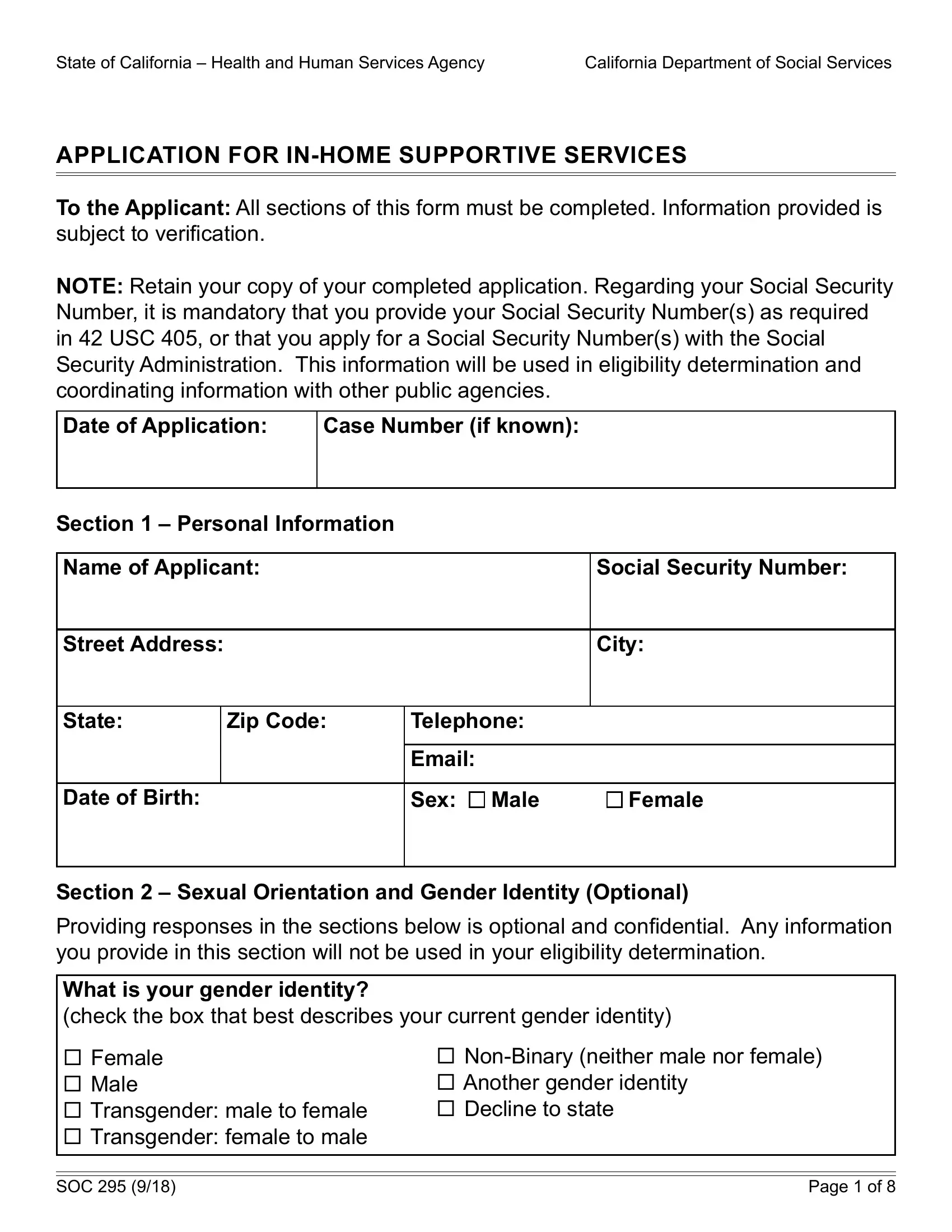
1. Start completing your 295 application social with a group of major blanks. Consider all the required information and make certain absolutely nothing is left out!
2. After performing the last part, go on to the next step and complete the essential particulars in these fields - What is your gender identity check, Female Male Transgender male to, NonBinary neither male nor female, SOC , and Page of .
3. Completing What sex was listed on your, Female Male, Straightheterosexual Gay or, Another sexual orientation Unknown, Section Veteran Information, Are you a Veteran, Are you a SpouseChild of a Veteran, Yes, Yes, and If YES give Veteran name and Claim is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
4. The subsequent paragraph will require your information in the subsequent places: Section SSISSP Information Do, Independent Living, Yes, Home of Another, Services being requested, Section Past IHSS Information, Have you received InHome, Yes, If Yes complete the following Date, Total Monthly Hours, and Name Used if different from above. Make sure you fill out all required details to go onward.
You can potentially make an error while filling out your Total Monthly Hours, and so make sure that you look again prior to deciding to submit it.
5. Lastly, this final segment is what you need to finish prior to using the document. The blanks at this point include the next: Name of Spouse, Birthdate, Social Security Number, Name of Parent Child Other, Birthdate, Social Security Number, Name of Parent Child Other, Birthdate, Social Security Number, Name of Parent Child Other, Birthdate, Social Security Number, and Name of Parent Child Other.
Step 3: Prior to finishing your file, make sure that all blank fields were filled in the proper way. Once you believe it's all fine, click “Done." Join FormsPal right now and instantly obtain 295 application social, available for download. Every modification made is conveniently saved , which means you can modify the pdf later on when required. With FormsPal, you can certainly fill out forms without stressing about data incidents or records being shared. Our protected system makes sure that your personal details are maintained safely.