
When working in the online tool for PDF editing by FormsPal, it is easy to fill in or change california participating physician application 2019 right here. Our editor is consistently evolving to give the very best user experience possible, and that's thanks to our dedication to constant enhancement and listening closely to user opinions. Starting is easy! All you should do is adhere to these basic steps below:
Step 1: First, access the editor by clicking the "Get Form Button" above on this page.
Step 2: As you start the PDF editor, you will get the form prepared to be filled in. Other than filling in various fields, you might also do several other things with the PDF, including putting on custom text, modifying the original textual content, inserting illustrations or photos, putting your signature on the PDF, and a lot more.
If you want to fill out this form, make certain you provide the necessary information in every single blank:
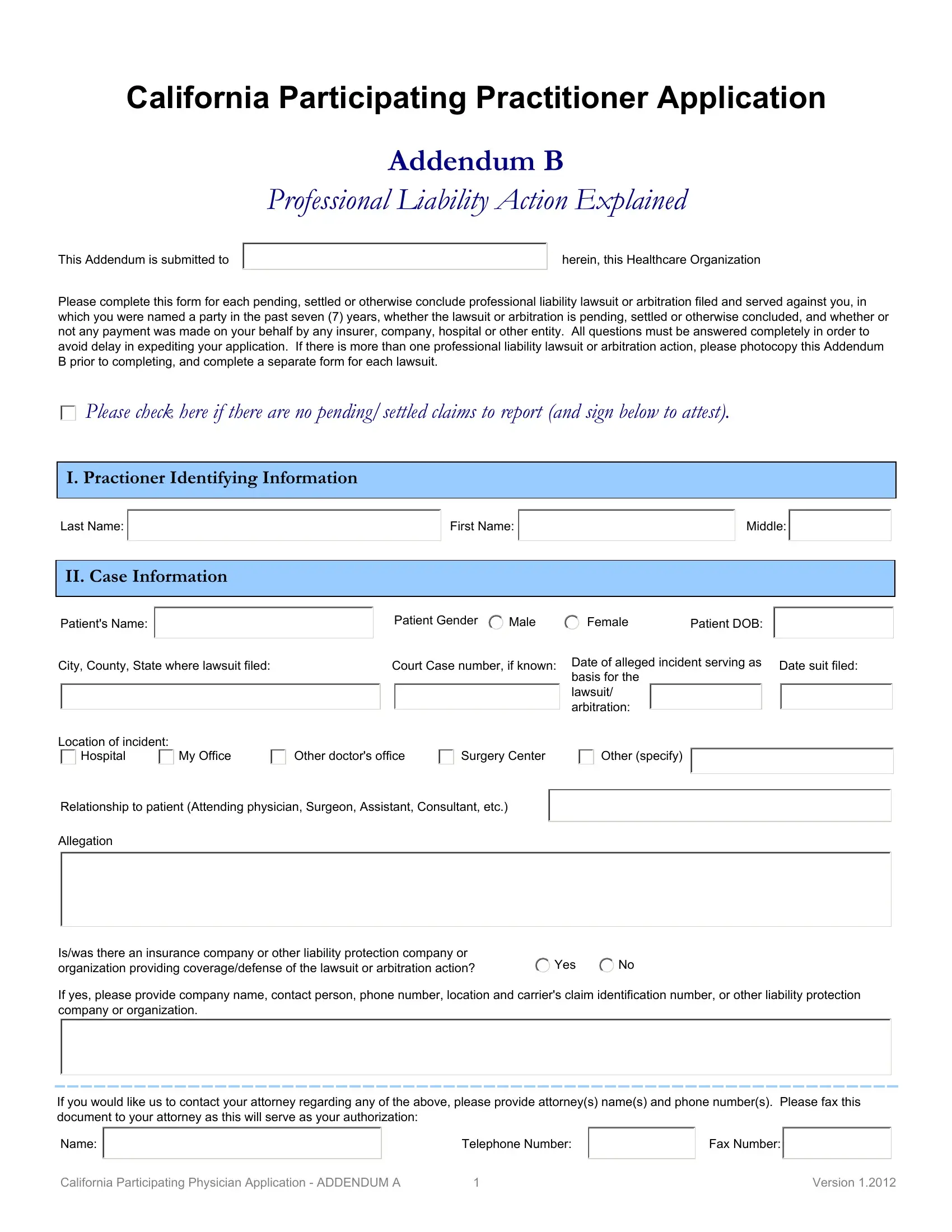
1. The california participating physician application 2019 usually requires particular details to be typed in. Be sure the subsequent blank fields are completed:
2. Just after this part is filled out, go on to type in the suitable details in these - City County State where lawsuit, Court Case number if known, Date of alleged incident serving, Date suit filed, Location of incident, Hospital, My Office, Other doctors office, Surgery Center, Other specify, Relationship to patient Attending, Allegation, Iswas there an insurance company, Yes, and If yes please provide company name.
People generally get some things incorrect while filling in Allegation in this section. Be certain to go over everything you enter right here.
3. This third stage is going to be straightforward - complete all of the fields in If you would like us to contact, Telephone Number, Fax Number, California Participating Physician, and Version to conclude this part.

4. To go forward, this form section requires typing in several blank fields. Examples include Lawsuitarbitration still ongoing, Judgment rendered and payment was, Amount paid on my behalf, Judgment rendered and I was found, Lawsuitarbitration settled and, Amount paid on my behalf, Lawsuitarbitration, Summarize the circumstances giving, Please include Condition and, and SUMMARY, which are key to moving forward with this process.
Step 3: Once you have looked over the information in the document, press "Done" to complete your document creation. Get your california participating physician application 2019 the instant you register here for a 7-day free trial. Readily view the pdf form within your personal cabinet, along with any modifications and adjustments automatically kept! FormsPal guarantees your data privacy by using a secure system that never saves or distributes any type of private information involved. Be confident knowing your files are kept safe each time you work with our services!